Archive for the ‘H7N9’ Category
The Centre for Health Protection (CHP) of the Department of Health is today (March 6) closely monitoring two additional human cases of avian influenza A(H7N9) in Guangxi.
Tuesday, March 7th, 2017
During March 2013–February 24, 2017, annual epidemics of avian influenza A(H7N9) in China resulted in 1,258 avian influenza A(H7N9) virus infections in humans being reported to the World Health Organization
Tuesday, March 7th, 2017
Increase in Human Infections with Avian Influenza A(H7N9) Virus During the Fifth Epidemic — China, October 2016–February 2017
Early Release / March 3, 2017 / 66
A. Danielle Iuliano, PhD1; Yunho Jang, PhD1; Joyce Jones, MS1; C. Todd Davis, PhD1; David E. Wentworth, PhD1; Timothy M. Uyeki, MD1; Katherine Roguski, MPH1; Mark G. Thompson, PhD1; Larisa Gubareva, PhD1; Alicia M. Fry, MD1; Erin Burns, MA1; Susan Trock, DVM1; Suizan Zhou, MPH2; Jacqueline M. Katz, PhD1; Daniel B. Jernigan, MD1 (View author affiliations)
During March 2013–February 24, 2017, annual epidemics of avian influenza A(H7N9) in China resulted in 1,258 avian influenza A(H7N9) virus infections in humans being reported to the World Health Organization (WHO) by the National Health and Family Planning Commission of China and other regional sources (1). During the first four epidemics, 88% of patients developed pneumonia, 68% were admitted to an intensive care unit, and 41% died (2). Candidate vaccine viruses (CVVs) were developed, and vaccine was manufactured based on representative viruses detected after the emergence of A(H7N9) virus in humans in 2013. During the ongoing fifth epidemic (beginning October 1, 2016),* 460 human infections with A(H7N9) virus have been reported, including 453 in mainland China, six associated with travel to mainland China from Hong Kong (four cases), Macao (one) and Taiwan (one), and one in an asymptomatic poultry worker in Macao (1). Although the clinical characteristics and risk factors for human infections do not appear to have changed (2,3), the reported human infections during the fifth epidemic represent a significant increase compared with the first four epidemics, which resulted in 135 (first epidemic), 320 (second), 226 (third), and 119 (fourth epidemic) human infections (2). Most human infections continue to result in severe respiratory illness and have been associated with poultry exposure. Although some limited human-to-human spread continues to be identified, no sustained human-to-human A(H7N9) transmission has been observed (2,3).
CDC analysis of 74 hemagglutinin (HA) gene sequences from A(H7N9) virus samples collected from infected persons or live bird market environments during the fifth epidemic, which are available in the Global Initiative on Sharing All Influenza Data (GISAID) database (4,5), indicates that A(H7N9) viruses have diverged into two distinct genetic lineages. Available fifth epidemic viruses belong to two distinct lineages, the Pearl River Delta and Yangtze River Delta lineage, and ongoing analyses have found that 69 (93%) of the 74 HA gene sequences to date have been Yangtze River Delta lineage viruses. Preliminary antigenic analysis of recent Yangtze River Delta lineage viruses isolated from infections detected in Hong Kong indicate reduced cross-reactivity with existing CVVs, whereas viruses belonging to the Pearl River Delta lineage are still well inhibited by ferret antisera raised to CVVs. These preliminary data suggest that viruses from the Yangtze River Delta lineage are antigenically distinct from earlier A(H7N9) viruses and from existing CVVs. In addition, ongoing genetic analysis of neuraminidase genes from fifth epidemic viruses indicate that approximately 7%–9% of the viruses analyzed to date have known or suspected markers for reduced susceptibility to one or more neuraminidase inhibitor antiviral medications. The neuraminidase inhibitor class of antiviral drugs is currently recommended for the treatment of human infection with A(H7N9) virus. Antiviral resistance can arise spontaneously or emerge during the course of treatment. Many of the A(H7N9) virus samples collected from human infections in China might have been collected after antiviral treatment had begun.
Although all A(H7N9) viruses characterized from the previous four epidemics have been low pathogenic avian influenza viruses, analysis of human (three) and environmental (seven) samples from the fifth epidemic demonstrate that these viruses contain a four–amino acid insertion in a host protease cleavage site in the HA protein that is characteristic of highly pathogenic avian influenza (HPAI) viruses. Chinese authorities are investigating and monitoring closely for outbreaks of HPAI A(H7N9) among poultry.
Since April 2013, the Influenza Risk Assessment Tool has been used by CDC to assess the risk posed by certain novel influenza A viruses. Although the current risk to the public’s health from A(H7N9) viruses is low, among the 12 novel influenza A viruses evaluated with this tool, A(H7N9) viruses have the highest risk score and are characterized as posing moderate–high potential pandemic risk (6). Experts from the World Health Organization (WHO) Global Influenza Surveillance and Response System (GISRS) met in Geneva, Switzerland, February 27–March 1, 2017, to review available epidemiologic and virologic data related to influenza A(H7N9) viruses to evaluate the need to produce additional CVVs to maximize influenza pandemic preparedness. Two additional H7N9 CVVs were recommended for development: a new CVV derived from an A/Guangdong/17SF003/2016-like virus (HPAI), which is a highly pathogenic virus from the Yangtze River Delta lineage; and a new CVV derived from A/Hunan/2650/2016-like virus, which is a low pathogenic virus also from the Yangtze River Delta lineage (1). At this time, CDC is preparing a CVV derived from an A/Hunan/2650/2016-like virus using reverse genetics. Further preparedness measures will be informed by ongoing analysis of genetic, antigenic, and epidemiologic data and how these data impact the risk assessment. CDC will continue to work closely with the Chinese Center for Disease Control and Prevention to support the response to this epidemic.
Guidance for U.S. clinicians who might be evaluating patients with possible H7N9 virus infection and travelers to China is available online (https://www.cdc.gov/flu/avianflu/h7n9-virus.htm).
References
World Health Organization. Antigenic and genetic characteristics of zoonotic influenza viruses and development of candidate vaccine viruses for pandemic preparedness, March 2017. Geneva, Switzerland: World Health Organization; 2017. http://www.who.int/influenza/vaccines/virus/201703_zoonotic_vaccinevirusupdate.pdf?ua=1
Xiang N, Li X, Ren R, et al. Assessing change in avian influenza A(H7N9) virus infections during the fourth epidemic—China, September 2015–August 2016. MMWR Morb Mortal Wkly Rep 2016;65:1390–4. CrossRef PubMed
Zhou L, Ren R, Yang L, et al. Sudden increase in human infection with avian influenza A(H7N9) virus in China, September–December 2016. Western Pac Surveill Response J 2017;8. CrossRef
Elbe S, Buckland-Merrett G. Data, disease and diplomacy: GISAID’s innovative contribution to global health. Global Challenges 2017;1:33–46. CrossRef
Federal Republic of Germany. The GISAID initiative. http://platform.gisaid.org/epi3/start
CDC. Influenza risk assessment tool (IRAT). Atlanta, GA: US Department of Health and Human Services, CDC; 2017. https://www.cdc.gov/flu/pandemic-resources/national-strategy/risk-assessment.htm
Top
Suggested citation for this article: Iuliano AD, Jang Y, Jones J, et al. Increase in Human Infections with Avian Influenza A(H7N9) Virus During the Fifth Epidemic — China, October 2016–February 2017. MMWR Morb Mortal Wkly Rep. ePub: 3 March 2017. DOI: http://dx.doi.org/10.15585/mmwr.mm6609e2.
U.S. officials say of all emerging influenza viruses, H7N9 currently poses the greatest risk of a pandemic threat if it evolves to spread readily from human to human.
Sunday, March 5th, 2017“….Centers for Disease Control and Prevention officials are developing a vaccine that would target a newly evolving version of the virus….”
H7N9: 21 more fall ill in China over past week
Saturday, March 4th, 2017CHP notified of human cases of avian influenza A(H7N9) in Mainland
The Centre for Health Protection (CHP) of the Department of Health today (March 3) received notification from the National Health and Family Planning Commission that 21 additional human cases of avian influenza A(H7N9), including three deaths, were recorded from February 24 to March 2. The CHP strongly urges the public to maintain strict personal, food and environmental hygiene both locally and during travel.
The 17 male and four female patients, aged from 10 to 77, had their onset from February 10 to 27. The cases were from Guangdong (six cases), Anhui (four cases), Jiangsu (three cases), two cases each in Guangxi and Jiangxi, and one case each in Hubei, Hunan, Shanghai and Zhejiang. Among them, 18 were known to have exposure to poultry or poultry markets.
Of note, according to the surveillance of the Guangdong Provincial Center for Disease Control and Prevention, from February 22 to 28, among 855 environmental samples collected from 89 markets in various areas in Guangdong, 83 samples from 27 markets tested positive for H7 virus, i.e. about 30 per cent of the markets in Guangdong and 9.7 per cent of the samples were positive.
Travelers to the Mainland or other affected areas must avoid visiting wet markets, live poultry markets or farms. They should be alert to the presence of backyard poultry when visiting relatives and friends. They should also avoid purchase of live or freshly slaughtered poultry, and avoid touching poultry/birds or their droppings. They should strictly observe personal and hand hygiene when visiting any place with live poultry.
Travelers returning from affected areas should consult a doctor promptly if symptoms develop, and inform the doctor of their travel history for prompt diagnosis and treatment of potential diseases. It is essential to tell the doctor if they have seen any live poultry during travel, which may imply possible exposure to contaminated environments. This will enable the doctor to assess the possibility of avian influenza and arrange necessary investigations and appropriate treatment in a timely manner.
While local surveillance, prevention and control measures are in place, the CHP will remain vigilant and work closely with the World Health Organization and relevant health authorities to monitor the latest developments.
The CHP’s Port Health Office conducts health surveillance measures at all boundary control points. Thermal imaging systems are in place for body temperature checks on inbound travellers. Suspected cases will be immediately referred to public hospitals for follow-up.
The display of posters and broadcasting of health messages in departure and arrival halls as health education for travellers is under way. The travel industry and other stakeholders are regularly updated on the latest information.
The public should maintain strict personal, hand, food and environmental hygiene and take heed of the advice below while handling poultry:
- Avoid touching poultry, birds, animals or their droppings;
- When buying live chickens, do not touch them and their droppings. Do not blow at their bottoms. Wash eggs with detergent if soiled with faecal matter and cook and consume them immediately. Always wash hands thoroughly with soap and water after handling chickens and eggs;
- Eggs should be cooked well until the white and yolk become firm. Do not eat raw eggs or dip cooked food into any sauce with raw eggs. Poultry should be cooked thoroughly. If there is pinkish juice running from the cooked poultry or the middle part of its bone is still red, the poultry should be cooked again until fully done;
- Wash hands frequently, especially before touching the mouth, nose or eyes, before handling food or eating, and after going to the toilet, touching public installations or equipment such as escalator handrails, elevator control panels or door knobs, or when hands are dirtied by respiratory secretions after coughing or sneezing; and
- Wear a mask if fever or respiratory symptoms develop, when going to a hospital or clinic, or while taking care of patients with fever or respiratory symptoms.
The public may visit the CHP’s pages for more information: the avian influenza page, the weekly Avian Influenza Report, global statistics and affected areas of avian influenza, the Facebook Page and the YouTube Channel.
US officials charged with preparing the country for influenza pandemics conclude that the stored H7N9 vaccine doesn’t adequately protect against a new branch of this virus family, and a new vaccine is needed.
Friday, March 3rd, 2017“…the Biomedical Advanced Research and Development Authority, or BARDA, said the H7N9 vaccine in the [US Strategic National Stockpile (SNS)] would not fend off a new family of these viruses that has emerged in China, known as the eastern or Yangtze River Delta lineage of the viruses….”
- The H7N9 virus is evolving and has essentially split into two groups that are now different enough that vaccine for one might not protect very well against viruses from the other.
- The US stockpile currently contains enough vaccines to inoculate about 12 million people against the older lineage of H7N9, the southern or Pearl River Delta viruses.
- The vaccines in the pandemic flu stockpile are intended to protect first responders in the case one of the highest-risk bird flu viruses triggers a pandemic. BARDA’s policy is to maintain enough vaccine for each of these top threats to be able to vaccinate 20 million people. As each person would need both a primer and a booster dose, that means 40 million doses of vaccine for each viral threat.
“The World Health Organization’s (WHO’s) flu vaccine advisory group today recommended changing one strain—the 2009 H1N1 component—for the Northern Hemisphere’s 2017-18 flu season……Also, the advisors reviewed the latest genetic information about recent avian and other zoonotic flu viruses and recommended two new candidate vaccine viruses for H7N9 avian flu, plus three new ones for other potential pandemic threats….”
Friday, March 3rd, 2017“…..The WHO recommends the following for the Northern Hemisphere’s trivalent vaccines:
- For H1N1, an A/Michigan/45/2015-like virus
- For H3N2, an A/Hong Hong/4801/2014-like virus
- For B, Brisbane/60/2008-like virus (belonging to the Victoria lineage)
For quadrivalent versions that contain two influenza B strains, the WHO experts recommended adding Phuket/3073/2013-like virus, a Yamagata lineage virus that is the second B component of quadrivalent vaccines for both the Southern Hemisphere’s past and the Northern Hemisphere’s current season….”

“…..Today the group said that recent H7N9 viruses fall into the Yangtze River Delta (YRD) or Pearl River Delta (PRD) hemagglutinin lineages, and that two existing candidate vaccine viruses don’t seem to protect against recent YRD-lineage viruses. They proposed a new candidate vaccine virus to protect against those viruses.
Also, they said the newly identified highly pathogenic H7N9 viruses isolated from poultry and people are genetically and antigenically distinct from other H7N9 viruses, including recommended candidate strain, including the newly proposed one. Therefore, the group recommended a new candidate vaccine virus to protect against the highly pathogenic H7N9 strain.
The group also recommended three other candidate pandemic vaccine viruses, two against recent variant H1N1 strains and one against the recent H5N6 virus circulating in Japan and South Korea……”

China’s Prime Minister urged local authorities to shut down live poultry markets in places affected by the H7N9 bird flu virus which killed 79 people in January.
Friday, February 24th, 2017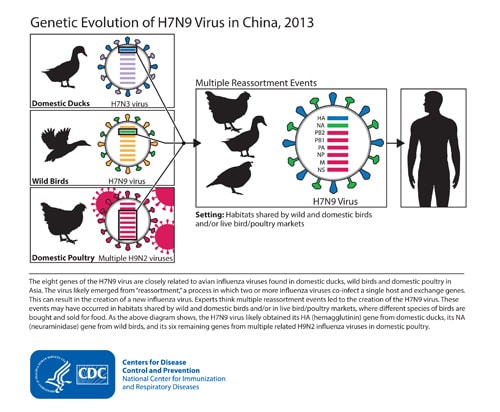

China: 2 more H7N9 infections in humans; Officials urge doctors to start antiviral treatment early, preferably within 48 hours of symptom onset, without waiting for influenza test results.
Wednesday, February 22nd, 2017National Health Commission on Strengthening the Medical Treatment of H7N9 Avian Influenza: “early detection, early reporting, early diagnosis, early treatment”
H7N9: Analysis of virus samples from China and Taiwan hint at mutations including resistance to the antiviral class of drugs known as neuraminidase inhibitors
Tuesday, February 21st, 2017
WHO: The burgeoning number of H7N9 cases this season now account for a third of all cases reported since the outbreak began in 2013.
Tuesday, February 21st, 2017Human infection with avian influenza A(H7N9) virus – China
Between 19 January and 14 February 2017, a total of 304 additional laboratory-confirmed cases of human infection have been reported to WHO from mainland China though the China National IHR focal point.
On 19 January 2017, the National Health and Family Planning Commission of China (NHFPC) notified WHO of 111 additional laboratory-confirmed cases of human infection with avian influenza A(H7N9) virus. On 24 January 2017, the NHFPC notified WHO of 31 additional laboratory-confirmed cases of human infection with avian influenza A(H7N9) virus. On 30 January 2017, the NHFPC notified WHO of 41 additional laboratory-confirmed cases of human infection with avian influenza A(H7N9) virus. On 7 February 2017, the NHFPC notified WHO of 52 additional laboratory-confirmed cases of human infection with avian influenza A(H7N9) virus. On 14 February 2017, the NHFPC notified WHO of 69 additional laboratory-confirmed cases of human infection with avian influenza A(H7N9) virus.
Details of the cases
Between 19 January and 14 February 2017, the NHFPC reported a total of 304 human cases of infection with avian influenza A(H7N9). Onset dates range from 13 December 2016 to 9 February 2017. Of these 304 cases, 86 are female (28%). Cases range in age from 3 to 85 years, with a median age of 58 years. The cases are reported from Jiangsu (67), Zhejiang (53), Guangdong (32), Anhui (31), Jiangxi (27), Hunan (26), Fujian (20), Hubei (20), Sichuan (6), Guizhou (4), Henan (4), Shandong (4), Shanghai (3), Liaoning (2), Yunnan (2), Beijing (1), Hebei (1), and Guangxi (1).
At the time of notification, there were 36 deaths, two cases had mild symptoms and 82 cases were diagnosed as either pneumonia (34) or severe pneumonia (48). The clinical presentations of the other 184 cases are not available at this time. 144 cases reported exposure to poultry or live poultry market, 11 cases have no clear exposure to poultry or poultry-related environments. 149 cases are under investigation.
Two clusters of two-person were reported:
- A 22-year-old female (mother of 3-year-old girl case who had symptom onset on 29 January 2017, died on 7 February 2017) reported from Yunnan province. She had developed symptom on 4 February 2017. She took care of her daughter during her daughter was sick. Both are reported to expose to poultry in Jiangxi province.
- A 45-year-old female (previously reported on 9 January) from Sihui city, Guangdong province. She had symptom onset on 17 December 2016, and died on 24 December 2016. She was exposed to poultry. Another case was a 43-year-old female from Guangzhou city, Guangdong province. She had symptom onset on 30 December 2016 and was admitted to hospital on the same day. She is the sister of the 45-year old female described above. She took care of her hospitalized sister but also had exposure to poultry. At the time of reporting, she was suffering from pneumonia.
While common exposure to poultry is likely, human to human transmission cannot be ruled out.
To date, a total of 1222 laboratory-confirmed human infections with avian influenza A(H7N9) virus have been reported through IHR notification since early 2013.
Public health response
Considering the increase in the number of human infections with avian influenza A(H7N9) since December 2016, the Chinese government has enhanced measures such as:
- Strengthened early diagnosis and early treatment, treatment of severe cases to reduce occurrence of severe cases and deaths.
- Convened meetings to further deploy prevention and control measures.
- Conducted public risk communication and sharing information with the public.
- The NHFPC strengthened epidemic surveillance, conducted timely risk assessment and analysed the information for any changes in epidemiology.
- The NHFPC requested local NHFPCs to implement effective control measures on the source of outbreaks and to minimize the number of affected people.
- The NHFPC, joined by other departments such as agriculture, industry and commerce, Food and Drug Administration, re-visited Jiangsu, Zhejiang, Anhui and Guangdong provinces where more cases occurred for joint supervision. The affected provinces have also strengthened multisectoral supervision, inspection and guidance on local surveillance, medical treatment, prevention and control and promoted control measures with a focus on live poultry market management control.
- Relevant prefectures in Jiangsu province have closed live poultry markets in late December 2016 and Zhejiang, Guangdong and Anhui provinces have strengthened live poultry market regulations.
WHO risk assessment
While similar sudden increases in the number of human avian influenza A(H7N9) cases identified have been reported in previous years the number of cases reported during this season is exceeding previous seasons. The number of human cases with onset from 1 October 2016 accounts for nearly one-third of all the human cases of avian influenza A(H7N9) virus infection reported since 2013.
However, human infections with the avian influenza A(H7N9) virus remain unusual. Close observation of the epidemiological situation and further characterization of the most recent human viruses are critical to assess associated risk and to adjust risk management measures timely.
Most human cases are exposed to avian influenza A(H7N9) virus through contact with infected poultry or contaminated environments, including live poultry markets. Since the virus continues to be detected in animals and environments, and live poultry vending continues, further human cases can be expected. Additional sporadic human cases may be also expected in previously unaffected provinces as it is likely that this virus circulates in poultry of other areas of China without being detected.
Although small clusters of human cases with avian influenza A(H7N9) virus have been reported including those involving healthcare workers, current epidemiological and virological evidence suggests that this virus has not acquired the ability of sustained transmission among humans. Therefore the likelihood of further community level spread is considered low.
WHO advice
WHO advises that travellers to countries with known outbreaks of avian influenza should avoid, if possible, poultry farms, contact with animals in live bird markets, entering areas where poultry may be slaughtered, or contact with any surfaces that appear to be contaminated with faeces from poultry or other animals. Travellers should also wash their hands often with soap and water, and follow good food safety and good food hygiene practices.
WHO does not advise special screening at points of entry with regard to this event, nor does it currently recommend any travel or trade restrictions. As always, a diagnosis of infection with an avian influenza virus should be considered in individuals who develop severe acute respiratory symptoms while travelling in or soon after returning from an area where avian influenza is a concern.
WHO encourages countries to continue strengthening influenza surveillance, including surveillance for severe acute respiratory infections (SARI) and influenza-like illness (ILI) and to carefully review any unusual patterns, ensure reporting of human infections under the IHR (2005), and continue national health preparedness actions.