Archive for May, 2016



Tropical Cyclone Roanu lashed the coast of Bangladesh with heavy winds and sheets of rain, killing at least 21 people and forcing the evacuation of half a million residents.
Sunday, May 22nd, 2016
The Indian Meteorological Department has forecast a severe heat wave for parts of western India through Saturday. Extreme heat was also forecast across central and northern India into next week.
Saturday, May 21st, 2016
WHO: Zika virus strain imported from the Americas to Cabo Verde
Saturday, May 21st, 201620 MAY 2016 | BRAZZAVILLE – Sequencing of the virus in Cabo Verde by Institut Pasteur, Dakar confirms that the Zika virus currently circulating in Cabo Verde is the same as the one circulating in the Americas – the Asian type- and was most likely imported from Brazil. This is the first time that the Zika strain responsible for the outbreaks linked to neurological disorders and microcephaly has been detected in Africa.

“The findings are of concern because it is further proof that the outbreak is spreading beyond South America and is on the doorstep of Africa. This information will help African countries to re-evaluate their level of risk and adapt and increase their levels of preparedness,” said Dr Matshidiso Moeti, WHO Regional Director for Africa.
As a first step, these countries should heighten risk communication to pregnant women to raise awareness of complications associated with the Asian type of Zika virus and promote protection steps to avoid mosquito bites as well as sexual transmission. In addition, countries should increase their surveillance for Zika transmission and congenital malformations, such as microcephaly, as well as Guillain-Barré syndrome.
Activated since February 2016, WHO Zika Virus Disease Incident Management System in Brazzaville and at Headquarters will continue to review existing risk assessments, increase surveillance, and assess laboratory testing capacity and support community engagement and risk communications in priority countries. In addition, WHO and its partners will support the countries in the African region to step up preparedness efforts for early detection, confirmation and management of potential complications related to Zika infection. The response will build on investments in strengthened systems made in West Africa during the Ebola emergency.
Zika in Cabo Verde
As of 8 May 2016, there have been 7557 suspected cases of Zika in Cabo Verde. Three cases of microcephaly have been reported from Cabo Verde with one case reported by the U.S. Centers for Disease Control and Prevention (CDC) after being delivered in the United States. So far, no case of Guillain-Barre Syndrome (GBS) has been reported from Cabo Verde.
Characteristics and outcomes of patients with chikungunya virus (CHIKV) infection admitted to an ICU in the Western Hemisphere
Saturday, May 21st, 2016Crosby L, Perreau C, Madeux B, Cossic J, Armand C, Herrmann-Storke C, Najioullah F, Valentino R, Thiery G, Severe ´ manifestations of Chikungunya virus in critically ill patients during the 2013- 2014 Caribbean outbreak., International Journal of Infectious Diseases (2016), http://dx.doi.org/10.1016/j.ijid.2016.05.010
- “Severe manifestations of Chikungunya virus infection affected a small number of patients compared to the entire infected population.
- Most patients had previous underlying diseases and presented with acute exacerbations triggered by Chikungunya virus infection.
- Encephalitis, Guillain-Barré syndrome and severe sepsis could to be directly related to Chikungunya virus.”
WHO has been notified of at least 38 suspected cases of Lassa fever in Liberia.so far this year
Saturday, May 21st, 2016Lassa Fever – Liberia

Since 1 January 2016, WHO has been notified of at least 38 suspected cases of Lassa fever in Liberia.
Suspected cases were reported from 6 prefectures: Bong (17 cases, including 9 deaths), Nimba (14 cases, including 6 deaths), Gbarpolu (4 cases), Lofa (1 case), Margibi (1 case) and Montserrado (1 case).
Between 1 January and 3 April 2016, samples from 24 suspected cases were received for laboratory testing. Of these 24 suspected cases, 7 are reported to have tested positive for Lassa fever:
- 2 cases were identified by polymerase chain reaction (PCR);
- 2 cases were identified through the detection of IgM antibodies using enzyme-linked immunosorbent assay (ELISA);
- 2 cases were identified through the detection of Lassa virus antigens using ELISA;
- information on the type of testing employed to identify the seventh case is not currently available.
All the Lassa fever confirmed cases tested negative for Ebola virus disease. Since there are no designated laboratories in Liberia that can test samples for Lassa fever by PCR, specimens are currently sent for testing to Kenema, Sierra Leone.
Public health response
To date, 134 contacts have completed the 21-day follow-up period. A total of 17 additional contacts are being monitored. None of these contacts have so far developed symptoms.
Appropriate outbreak response measures, including case management, infection prevention and control, community engagement and health education, have been put in place by the national authorities with the support of WHO and partner organizations.
WHO risk assessment
Lassa fever is endemic in Liberia and causes outbreaks almost every year in different parts of the country. Based on experiences from previous similar events, it is expected that additional cases will be reported.
Although occasional travel-associated cases of Lassa fever have been reported in the past (see DON published on 27 and 8 April 2016), the risk of disease spread from Liberia to non-endemic countries is considered to be low. WHO continues to monitor the epidemiological situation and conduct risk assessments based on the latest available information.
WHO advice
Considering the seasonal flare ups of cases during this time of the year, countries in West Africa that are endemic for Lassa fever are encouraged to strengthen their related surveillance systems.
Health-care workers caring for patients with suspected or confirmed Lassa fever should apply extra infection control measures to prevent contact with the patient’s blood and body fluids and contaminated surfaces or materials such as clothing and bedding. When in close contact (within 1 metre) of patients with Lassa fever, health-care workers should wear face protection (a face shield or a medical mask and goggles), a clean, non-sterile long-sleeved gown, and gloves (sterile gloves for some procedures).
Laboratory workers are also at risk. Samples taken from humans and animals for investigation of Lassa virus infection should be handled by trained staff and processed in suitably equipped laboratories under maximum biological containment conditions.
The diagnosis of Lassa fever should be considered in febrile patients returning from areas where Lassa fever is endemic. Health-care workers seeing a patient suspected to have Lassa fever should immediately contact local and national experts for advice and to arrange for laboratory testing.
WHO does not recommend any travel or trade restriction to Liberia based on the current information available.
Key facts
- Lassa fever is an acute viral haemorrhagic illness of 2-21 days duration that occurs in West Africa.
- The Lassa virus is transmitted to humans via contact with food or household items contaminated with rodent urine or faeces.
- Person-to-person infections and laboratory transmission can also occur, particularly in hospitals lacking adequate infection prevent and control measures.
- Lassa fever is known to be endemic in Benin, Ghana, Guinea, Liberia, Mali, Sierra Leone, and Nigeria, but probably exists in other West African countries as well.
- The overall case-fatality rate is 1%. Observed case-fatality rate among patients hospitalized with severe cases of Lassa fever is 15%.
- Early supportive care with rehydration and symptomatic treatment improves survival.
Symptoms of Lassa fever
The incubation period of Lassa fever ranges from 6–21 days.
The onset of the disease, when it is symptomatic, is usually gradual, starting with fever, general weakness, and malaise.
After a few days, headache, sore throat, muscle pain, chest pain, nausea, vomiting, diarrhoea, cough, and abdominal pain may follow.
In severe cases facial swelling, fluid in the lung cavity, bleeding from the mouth, nose, vagina or gastrointestinal tract and low blood pressure may develop.
Parts of EgyptAir Flight MS804 and passenger belongings have been discovered near Alexandria
Friday, May 20th, 2016
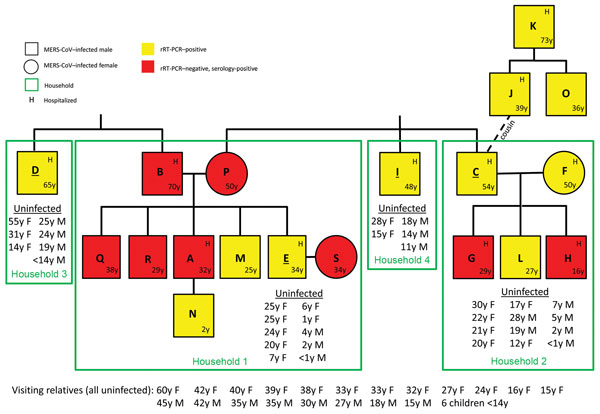
MERS-CoV Transmission in an Extended Family, Saudi Arabia, 2014
Friday, May 20th, 2016CDC- Emerging Infectious Diseases
Abstract
“Risk factors for human-to-human transmission of…MERS-CoV are largely unknown. After MERS-CoV infections occurred in an extended family in Saudi Arabia in 2014, relatives were tested by using….rRT-PCR and serologic methods. Among 79 relatives, 19 (24%) were MERS-CoV positive; 11 were hospitalized, and 2 died. Eleven (58%) tested positive by rRT-PCR; 8 (42%) tested negative by rRT-PCR but positive by serology. Compared with MERS-CoV–negative adult relatives,
- MERS-CoV–positive adult relatives were older and more likely to be male and to have chronic medical conditions.
- Risk factors for household transmission included sleeping in an index patient’s room and touching respiratory secretions from an index patient.
- Casual contact and simple proximity were not associated with transmission.
- Serology was more sensitive than standard rRT-PCR for identifying infected relatives, highlighting the value of including serology in future investigations.”