Archive for February, 2018
Heavy Rain and Flooding in the Southern Plains to the Great Lakes
Wednesday, February 21st, 2018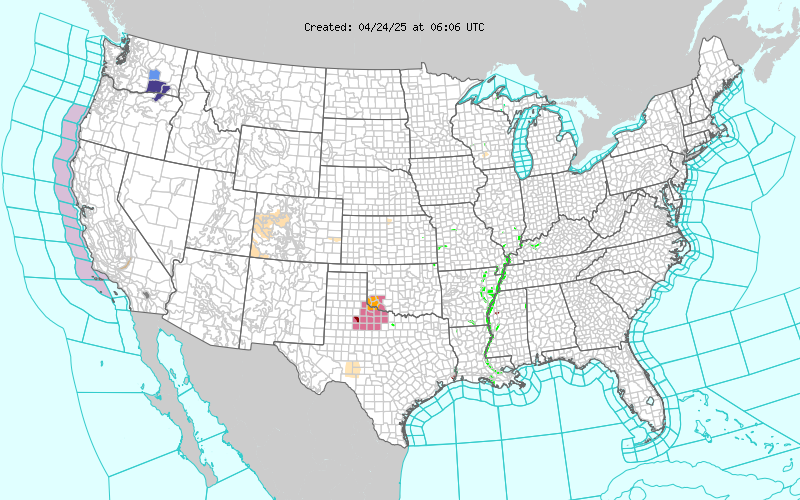
Short Range Forecast Discussion
NWS Weather Prediction Center College Park MD
300 AM EST Wed Feb 21 2018
Valid 12Z Wed Feb 21 2018 – 12Z Fri Feb 23 2018
…Cold temperatures across the West and warm across the East with a
continuing active wet pattern across the central U.S…
Excessive rain and areal flooding will continue from portions of the
Southern Plains to the Great Lakes Region as warm Gulf moisture lifts
northward along a slow moving frontal boundary. Cold air behind the front
will allow for snow,or possible a wintry mix/ freezing rain. Numerous
Winter Weather Advisories are in effect from central Texas to Illinois.
Minor flooding is being observed across western portions of the Tennessee
and Mid-Mississippi Valleys. Several locations across Lower Great
Lakes/western Ohio Valley already have minor to moderate flooding, any
additional rainfall will likely exacerbate the situation.
Temperatures across much of the Eastern Seaboard will be above-to-well
above normal for late February. Widespread highs in the 70s with some
lower 80s are expected, and this has the potential to set record highs.
These late Spring-like temperatures will be short-lived. The strong front
over the central U.S. will finally cross the Central/Northern Appalachians
and cold air will spill into the Northeast and Mid-Atlantic regions by the
end of the week.
Upper-level energy will move southward though the Pacific Northwest will
spread snow spread from the coast inland and south to northern California.
Much of the West will have temperatures warmer than seasonal average
Campbell
Graphics available at www.wpc.ncep.noaa.gov/basicwx/basicwx_ndfd.php

he Saudi Arabian Ministry of Health (MOH) confirmed one new case of MERS-CoV on Feb 17.
Tuesday, February 20th, 2018
PAHO: Yellow Fever Update in the Americas
Tuesday, February 20th, 2018Situation summary in the Americas
Between January 2016 and January 2018, seven countries and territories of the Region of the Americas reported confirmed cases of yellow fever: the Plurinational State of Bolivia, Brazil, Colombia, Ecuador, French Guiana, Peru, and Suriname. The number of human cases and epizootics collectively reported in this period in the Region of the Americas is the highest observed in decades.
Since the 12 January 2018 Epidemiological Update on Yellow Fever published by the Pan American Health Organization / World Health Organization (PAHO/WHO), Brazil and Peru had reported new yellow fever cases; following is a summary of the situation in both countries.
In Brazil, between 1 July 2017 and 15 February 2018, there were 409 confirmed human cases of yellow fever, including 118 deaths; this figure is lower than what was reported for the same period of the previous year (532 cases including 166 deaths) (Figure 1). In decreasing order, confirmed cases were reported in the states of São Paulo (183 cases, including 46 deaths), Minas Gerais (157 cases, including 44 deaths), Rio de Janeiro (68 cases, including 27 deaths), and in the Federal District (1 fatal case).
During the first four weeks of 2018, a major increase of yellow fever confirmed cases has been observed and reported cases in the states of Sao Paulo and Rio de Janeiro have significantly exceeded the numbers reported in the preceding season, 2016/2017, with cases reported in areas near major cities. In São Paulo, 57% of the confirmed cases had the probable place of infection in a rural area of the municipality of Mairiporã, located 15 kilometers from the northern area of São Paulo city. In Rio de Janeiro, 45% of the confirmed cases are residents of the municipalities of Valença and Teresópolis, the latter located 96 kilometers from the city of Rio de Janeiro. In Minas Gerais, 47% of the confirmed cases reside in the municipalities located to the south and southeast of the city of Belo Horizonte; where no human cases had been detected during the outbreak in the 2016/2017 seasonal period. The probable sites of infection of all the confirmed cases correspond to areas with documented epizootics in non-human primates (NHP).
In addition, two confirmed yellow fever cases (European citizens) have been reported among unvaccinated travelers who had stayed in municipalities of Brazil considered at-risk for yellow fever and where the circulation of the virus has previously been reported.
On 15 February 2018, the Brazil Ministry of Health reported the detection of yellow fever virus in Aedes albopictus mosquitoes captured in rural areas of two municipalities, Ituêta and Alvarenga, of Minas Gerais state in 2017 through an investigation carried out by the Evandro
Pan American Health Organization • http://www.paho.org/ • © PAHO/WHO, 2018
– 2 –
Chagas Institute. The significance of these findings requires further investigation particularly to confirm vector capacity for transmission.1
To date, there is no evidence that Aedes aegypti is implicated in the transmission.
Figure 1. Distribution of confirmed yellow fever cases by epidemiological week (EW). Brazil, 2016 – 2018
Source: Data published by the Ministry of Health of Brazil and reproduced by PAHO/WHO
With respect to epizootics in Brazil, between 1 July 2017 and 15 February 2018 a total of 3,481 epizootics were reported, representing a greater total than that which was reported during the 2016/2017 outbreak which had a total of 1,659 epizootics.
Of the 3,481 epizootics reported, 499 were confirmed for yellow fever, 1,242 were classified as undetermined (samples were not collected), 1,018 remain under investigation, and 722 were discarded. The state with the highest number of confirmed epizootics is São Paulo (Figure 2). Epizootics were also confirmed in the states of Espiritu Santo, Mato Grosso, Minas Gerais, Rio de Janeiro, and Tocantins. The epizootics occurred in 27 federal entities, including in municipalities that were previously considered as no at-risk for yellow fever.
The number of epizootics reported in the current season is greater than the total reported in the previous season. This situation is compounded by the fact that epizootics are occurring in areas very close to large urban settings such as Sao Paulo and Rio de Janeiro city. The map (Figure 3) shows the advancement of the epizootic wave towards the south of the state of São Paulo. If the epizootic wave repeats the same pattern observed a decade ago—the epizootic wave affected southeastern and southern Brazil and subsequently reached Argentina and Paraguay—this current epizootic wave could reach the neighboring countries again. As part of the response to the outbreak, federal and state authorities are conducting mass vaccination campaigns to immunize susceptible populations. As of 15 February 2018, preliminary results of the mass yellow fever vaccination campaign carried out by the Brazil health authorities – targeting 69 municipalities within the states of Rio de Janeiro (10 million persons in 15 municipalities) and São Paulo (10.3 million in 54 municipalities), indicate that 3.95 1 Brazil Ministry of Health press release, available at: http://bit.ly/2o9yNx4
Pan American Health Organization • http://www.paho.org/ • © PAHO/WHO, 2018
– 3 –
million persons have been vaccinated for yellow fever (3.6 million persons with fractional doses and 356,800 with standard doses). This figure represents 19.3% of the 20.5 million persons targeted for vaccination within the two states. Due to the low vaccination rate achieved during the campaign in Rio de Janeiro State (12% of the targeted population), state health authorities will extend the campaign and in São Paulo State (26% of the targeted population vaccinated) authorities are assessing the need to extend the campaign for several additional days. In Bahia, the campaign will begin on 19 February with a targeted population to vaccinate of 3.3 million persons in 8 municipalities.
Figure 2. Distribution of epizootics reported per EW. São Paulo, Brazil. EW 26 of 2016 to EW 5 of 2018.
Source: Data published by the São Paulo State Health Secretary, Brazil, and reproduced by PAHO/WHO
Figure 3. Confirmed human cases and municipalities with confirmed yellow fever epizootics. São Paulo, Brazil, July 2017 to 14 February 2018.
Pan American Health Organization • http://www.paho.org/ • © PAHO/WHO, 2018
– 4 –
In Peru, between EW 1 and 4 of 2018, three probable cases of yellow fever were reported, one of which was confirmed by laboratory. All three cases had no history of yellow fever vaccination.
The first two cases are residents of the city of Pucallpa in the Calleria district, Coronel Portillo Province, Ucayali department, an area considered at-risk for yellow fever. Both had onset of symptoms in EW2 of 2018. The first case died and the second case, spouse of the first case, was discharged and confirmed with yellow fever by Elisa IgM and RT-PCR techniques. The laboratory confirmed case has no history of having travelled outside of the city of Pucallpa; the investigation on the probable place of infection is ongoing accordingly.
The third case, is a resident of the Union Progreso, Inambari District, in the department of Madre de Dios, an area considered to be at-risk for yellow fever. Symptoms onset on EW 4 of 2018; the laboratory results are pending. This case works as a fluvial transporter between the towns of Laberinto, Colorado, and Unión Guacamayo where there are mining camps.
In Peru, between January and December of 2017, there were 14 yellow fever cases reported in 6 departments: 1 in Huánuco, 3 in Ayacucho, 1 in Cusco, 6 in Junín, 1 in Loreto, and 2 in San Martin.
Advice for national authorities
The occurrence of confirmed cases of yellow fever in unvaccinated travelers highlights the need for Member States to reinforce the dissemination of recommendations for international travelers. PAHO/WHO encourages Member States to continue efforts to immunize the at-risk populations and take the necessary actions to keep travelers informed and vaccinated, when heading to areas where yellow fever vaccination is recommended.
On 16 January 2018, the WHO published updated advice, titled, “Updates on yellow fever vaccination recommendations for international travelers related to the current situation in Brazil, information for international travelers,” available at: http://www.who.int/ith/updates/20180116/en/
Vaccination
The yellow fever vaccine is safe and affordable and provides effective immunity against the disease in the range of 80 to 100% of those vaccinated after 10 days and 99% immunity after 30 days. A single dose provides life-long protection against yellow fever disease. A booster dose of yellow fever vaccine is not needed.
Given the limitations on the availability of vaccines and with the aim of promoting the rational use, PAHO/WHO reiterates its recommendations to national authorities:
1. Conduct an assessment of vaccination coverage against yellow fever in areas at risk at the municipal level to guarantee at least 95% coverage2 among the resident population of these areas. 2 Pan American Health Organization. Regional immunization action plan. 54th Directing Council of PAHO, 67th session of the WHO Regional Committee for the Americas; 28 September – 1 October 2015; Washington (DC),
Pan American Health Organization • http://www.paho.org/ • © PAHO/WHO, 2018
– 5 –
2. Member States that are not currently experiencing outbreaks should not conduct yellow fever immunization campaigns. Priority should be given to the use of vaccines in susceptible populations and to avoid revaccination.
3. Ensure vaccination of all travelers to endemic areas at least 10 days before traveling.
4. Depending on vaccine availabilities, Member States should have a small stock that allows them to respond to outbreaks.
5. Postpone routine vaccination in children in non-endemic areas until sufficient vaccines are available. Once there is availability, catch-up campaigns should be conducted to complete vaccination schedules.
Precautions
It is recommended to individually assess the epidemiological risk of contracting disease when faced with the risk of an adverse event occurring in persons over 60 years who have not been previously vaccinated.
The vaccine can be offered to individuals with asymptomatic HIV infection with CD4+ counts ≥ 200 cells / mm3 requiring vaccination.
Pregnant women should be vaccinated in emergency epidemiological situations and following the explicit recommendations of health authorities.
Vaccination is recommended in nursing women who live in endemic areas, since the potential risk of transmitting the vaccine virus to the child is far lower than the benefits of breastfeeding.
For pregnant or lactating women traveling to areas with yellow fever transmission, vaccination is recommended when travel cannot be postponed or avoided. They should receive advice on the potential benefits and risks of vaccination to make an informed decision. The benefits of breastfeeding are superior to those of other nutritional alternatives.
The following people are usually excluded from yellow fever vaccination:
• Immunocompromised individuals (Including those with thymus disorders, symptomatic HIV, malignant neoplasms under treatment, and those that are receiving or have received immunosuppressive or immunomodulatory treatments, recent transplants, and current or recent radiation therapy).
• People with severe allergies to eggs and their derivatives.
United States. Washington (DC): PAHO; 2015. Available at: http://www2.paho.org/hq/index.php?option=com_content&view=article&id=13101&Itemid=42296&lang=en
Pan American Health Organization • http://www.paho.org/ • © PAHO/WHO, 2018
– 6 –
Related Links
Brazil Ministry of Health. Yellow Fever Reports. Available at: http://bit.ly/2sq3aV6
PAHO/WHO Yellow Fever. Available at: http://www.paho.org/hq/index.php?option=com_topics&view=rdmore&cid=5514&Ite mid=40784&lang=en
PAHO/WHO. Guidance on Laboratory Diagnosis of Yellow Fever Virus Infection. Available at: http://www.paho.org/hq/index.php?option=com_docman&task=doc_download&Item id=270&gid=38104&lang=en
PAHO/WHO. Requirements for the International Certificate of Vaccination or Prophylaxis (ICVP) with proof of vaccination against yellow fever. Available at: http://www.paho.org/hq/index.php?option=com_topics&view=article&id=69&Itemid=4 0784&lang=en
PAHO Health Emergencies Interactive Atlas and Maps. Available at: http://www.paho.org/hq/index.php?option=com_content&view=article&id=13224%3Ainteractive-atlas-and-maps&catid=3889%3Aaro-contents&Itemid=42337&lang=en
Syrian enclave: “….Medical organisations said at least four clinics and hospitals, including a maternity centre, were bombed on Monday, some of them multiple times, putting them out of service. An anaesthetist was killed in the attacks. ….”
Tuesday, February 20th, 2018A UC Davis-led program – PREDICT – discovers and detects viruses, many of which move between animals and people and can potentially trigger pandemics.
Tuesday, February 20th, 2018Department of Homeland Security: Austere Emergency Medical Support Field Guide.
Tuesday, February 20th, 2018E.U.’s Migrant Crisis Reaches Brussels
Monday, February 19th, 2018“…..Seeing unauthorized migration rise in Brussels last summer, the Belgian government ordered a series of heavy-handed raids on informal camps and homeless shelters. Those raids — along with falling temperatures — have largely succeeded in breaking up camps in public parks, and received wide popular support.
Even so, hundreds of Belgian families have reacted by inviting migrants into their homes. (Last month, the government proposed police raids on the houses of citizens suspected of sheltering unauthorized migrants.) Medical charities are providing food, clothes and assistance, and volunteers have set up shelters like the one where Mr. Khater sleeps, in a former office building. The total cost of sheltering one migrant is about 10 euros per night, organizers estimate…..”
Five killed & 5 wounded in an ISIS shooting at a church in Russia’s Dagestan.
Monday, February 19th, 2018
A fractional dose (1/5) of the 17DD yellow fever vaccine: Effective?
Monday, February 19th, 2018
“….In 2016, the response to a yellow fever outbreak in Angola and the Democratic Republic of Congo led to a global shortage of yellow fever vaccine. As a result, a fractional dose of the 17DD yellow fever vaccine (containing one fifth [0.1 ml] of the standard dose) was offered to 7.6 million children 2 years of age or older and nonpregnant adults in a preemptive campaign in Kinshasa. …………
A fractional dose of the 17DD yellow fever vaccine was effective at inducing seroconversion in most of the participants ….”
Venezuela: “I sold my hair to feed my girl.”
Sunday, February 18th, 2018“…..Venezuela is steeped in economic and political turmoil. Inflation last year surpassed 2,600 percent, according to opposition lawmakers, which has exacerbated severe shortages of food and medicine.……”