Archive for September, 2018

Measles in America: 6,629 confirmed cases, including 72 deaths
Tuesday, September 25th, 2018In 2018, as of 21 September, a total of 6,629 confirmed cases of measles, including 72 deaths, have been reported in 11 countries of the Region of the Americas:
Antigua and Barbuda (1 case),
Argentina (11 cases),
Brazil (1,735 cases, including 10 deaths),
Canada (22 cases),
Colombia (85 cases),
Ecuador (19 cases),
Guatemala (1 case),
Mexico (5 cases),
Peru (21 cases),
the United States of America (124 cases), and the
Bolivarian Republic of Venezuela (4,605 cases, including 62 deaths).
Diarrhea in 195 countries
Tuesday, September 25th, 2018“…..In 2016, diarrhoea was the eighth leading cause of death among all ages (1 655 944 deaths, 95% uncertainty interval [UI] 1 244 073–2 366 552) and the fifth leading cause of death among children younger than 5 years (446 000 deaths, 390 894–504 613). Rotavirus was the leading aetiology for diarrhoea mortality among children younger than 5 years (128 515 deaths, 105 138–155 133) and among all ages (228 047 deaths, 183 526–292 737). Childhood wasting (low weight-for-height score), unsafe water, and unsafe sanitation were the leading risk factors for diarrhoea, responsible for 80·4% (95% UI 68·2–85·0), 72·1% (34·0–91·4), and 56·4% (49·3–62·7) of diarrhoea deaths in children younger than 5 years, respectively. Prevention of wasting in 1762 children (95% UI 1521–2170) could avert one death from diarrhoea……”

Hospitals & Mass Shootings: What to do…….
Sunday, September 23rd, 2018At least 24 killed and 53 others injured in an attack on a military parade in Ahvaz, Iran
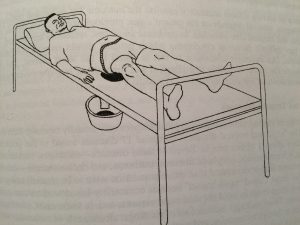
Saturday, September 22nd, 2018Tetanus in the wake of Florence
Saturday, September 22nd, 2018Pathogenesis
Clostridium tetani (C. tetani) spores usually enter the body through a wound or breach in the skin. Neonatal tetanus usually occurs because of umbilical stump infections. In the presence of anaerobic conditions, the spores germinate. The bacteria produce very potent toxins, most of which the blood stream and lymphatic system disseminate through the body. Toxins act at several sites within the central nervous system, including peripheral motor end plates, spinal cord, and brain, as well as in the sympathetic nervous system. Tetanus toxin causes the typical clinical manifestations of tetanus by interfering with the release of neurotransmitters and blocking inhibitor impulses. This leads to unopposed muscle contraction and spasm. Seizures may occur, and the autonomic nervous system may also be affected.
Risk Groups
Nearly all cases of tetanus in the United States today are among people who
- Have never received a tetanus vaccine
- Didn’t stay up to date on their 10-year booster shots
Tetanus Prevention after a Disaster
In most settings, a disaster does not increase the risk for tetanus. This includes earthquakes, hurricanes, floods, and tsunamis.
However, you can minimize the risk of tetanus among your patients who are disaster survivors and emergency responders by following routine vaccination recommendations and providing proper wound care.
Most reported cases occur in adults. From 2009–2015, more than 60% of the 197 reported cases were among people 20 through 64 years of age. In addition, a quarter of those reported cases were among people 65 years old or older. The risk of death from tetanus is highest among people 65 years old or older.
Diabetes, a history of immunosuppression, and intravenous drug use may be risk factors for tetanus. From 2009 through 2015, persons with diabetes was associated with 13% of all reported tetanus cases, and a quarter of all tetanus deaths. Intravenous drug users accounted for 6% of cases from 2009 through 2015.
Risk during Natural Disasters
In most settings, a disaster (e.g., earthquake, hurricane, flood, tsunami) does not increase the risk for tetanus. Minimize the risk of tetanus among your patients who are disaster survivors and emergency responders by following routine vaccination recommendations and providing proper wound care.
Symptoms and Diagnosis
Tetanus is a clinical syndrome without confirmatory laboratory tests. Characteristic symptoms of tetanus are painful muscular contractions, primarily of the masseter and neck muscles and secondarily of trunk muscles. Trismus, or lockjaw, is a common sign of tetanus (see generalized tetanus under Clinical Features). A common first sign suggestive of tetanus in older children and adults is abdominal rigidity, although rigidity is sometimes confined to the region of injury. Generalized spasms occur, frequently induced by sensory stimuli. History of an injury or apparent portal of entry may be lacking. The organism is rarely recovered from the site of infection.
Clinical Features
The incubation period ranges from 3 to 21 days, averaging about 10 days. In general, the further the injury site is from the central nervous system, the longer the incubation period. A shorter incubation period is associated with more severe disease, complications, and a higher chance of death. In neonatal tetanus, symptoms usually appear from 4 to 14 days after birth, averaging about 7 days.
There are three clinical forms of tetanus: generalized, localized, and cephalic.
Generalized Tetanus
Generalized tetanus is the most common form, accounting for more than 80% of cases. The most common initial sign is spasm of the muscles of the jaw or “lockjaw”. This may be followed by painful spasms in other muscle groups in the neck, trunk, and extremities and by generalized, seizure-like activity or convulsions in severe cases. Generalized tetanus can be accompanied by nervous system abnormalities, as well as a variety of complications related to severe spasm and prolonged hospitalization. The clinical course of generalized tetanus is variable and depends on the degree of prior immunity, the amount of toxin present, and the age and general health of the patient. Even with modern intensive care, generalized tetanus is associated with death rates of 10% to 20%.
Localized Tetanus
Localized tetanus is an unusual form of the disease consisting of muscle spasms in a confined area close to the site of the injury. Although localized tetanus often occurs in people with partial immunity and is usually mild, progression to generalized tetanus can occur.
Cephalic Tetanus
The rarest form, cephalic tetanus, is associated with lesions of the head or face and may also be associated with otitis media. The incubation period is short, usually 1 to 2 days. Unlike generalized and localized tetanus, cephalic tetanus results in flaccid cranial nerve palsies rather than spasm. Spasm of the jaw muscles may also be present. Like localized tetanus, cephalic tetanus can progress to the generalized form.
Complications of Tetanus
- Laryngospasms
- Fractures
- Hypertension
- Nosocomial infections
- Pulmonary embolism
- Aspiration pneumonia
- Death
Treatment
Tetanus is a medical emergency requiring hospitalization, immediate treatment with human tetanus immune globulin (TIG), agents to control muscle spasm, aggressive wound care, antibiotics, and a tetanus toxoid booster. If tetanus immune globulin is unavailable, Immune Globulin Intravenous (IGIV) can be used.
A patent airway should be maintained and, depending on the severity of disease, endotracheal intubation or tracheostomy and mechanically assisted respiration may be lifesaving. Sedation and muscle relaxant drugs should be used as indicated to control muscle spasms. Agents to control autonomic nervous system instability may be required. Initiate active immunization concurrently with treatment.
Treatment of tetanus cases with TIG
A single dose of human TIG is recommended for treatment of persons with tetanus. Although the optimal therapeutic dose has not been established, experts recommend 500 international units (IU), which appears to be as effective as higher doses ranging from 3,000 to 6,000 IU and causes less discomfort.
Available preparations must be administered intramuscularly; TIG preparations available in the United States are not licensed or formulated for intrathecal or intravenous use.
Infiltration of part of the dose locally around the wound is recommended (see Red Book), although its efficacy has not been proven.
If TIG is not available, IGIV can be used at a dose of 200 to 400 milligrams per kilogram (mg/kg). However, the Food and Drug Administration has not approved IGIV for this use. In addition, anti- tetanus antibody content varies from lot to lot.
Vaccination during Recovery
Tetanus disease does not result in tetanus immunity. Active immunization with a tetanus toxoid-containing vaccine should begin or continue as soon as the person’s condition has stabilized.
Wound Management for Tetanus Prevention
Risk of tetanus disease depends on the type and condition of the wound and immune status of the patient. The following steps should be taken to prevent tetanus:
- Assess the type of wound and provide appropriate wound care.
Wounds may be clean or contaminated and dirty, superficial or deep and penetrating. Dirty wounds pose an increased risk for tetanus. Wounds should be considered dirty if contaminated with dirt, soil, feces, or saliva (e.g., animal or human bites). Penetrating or puncture wounds are considered contaminated and may pose a higher risk for tetanus. Wounds containing devitalized tissue (e.g., necrotic or gangrenous wounds), frostbite, crush injuries, avulsion fractures, and burns are particularly conducive for proliferation of C. tetani. All wounds should be cleaned, dirt or foreign material removed, and necrotic material removed or debrided. - Evaluate the immunization status of the patient. Unvaccinated persons should start and complete a primary series with an age-appropriate tetanus toxoid-containing vaccine (DTaP, TdaP, or Td) as currently recommended by CDC.Persons with unknown or uncertain history of receiving previous prior doses tetanus toxoid-containing vaccines should be considered to have had no previous tetanus toxoid-containing vaccine and a primary series should be completed. This is because early doses of toxoid may not induce adequate immunity, but only prime the immune system.Persons who have completed a 3-dose primary tetanus vaccination series:
- If the last dose of a tetanus toxoid-containing vaccine was received less than 5 years earlier, they are considered protected against tetanus and do not require another dose of tetanus toxoid-containing vaccine as part of the current wound management.
- If the last dose of a tetanus toxoid-containing vaccine was received 5 or more years earlier, then a booster dose of an age-appropriate tetanus toxoid-containing vaccine should be administered.
- Rarely have cases of tetanus occurred in persons with a documented primary series of tetanus toxoid.
- Assess need for administering TIG for prophylaxis.
TIG provides temporary immunity by directly providing antitoxin. TIG can only help remove unbound tetanus toxin but cannot neutralize toxin that is already bound to nerve endings. Persons who have contaminated and dirty wounds and are either unvaccinated or have not received a primary series of tetanus toxoid-containing vaccines should receive TIG for prophylaxis. The dose of TIG for prophylaxis is 250 IU administered intramuscularly. People with HIV infection or severe immunodeficiency who have contaminated wounds (including minor wounds) should also receive TIG, regardless of their history of tetanus immunizations. - Do not use antibiotics for prophylaxis against tetanus.
Antibiotic prophylaxis against tetanus is not recommended, but wounds should be observed for signs of infection and promptly treated if signs of infection are detected.
Guide to Tetanus Prophylaxis with TIG in Routine Wound Management
| History of adsorbed tetanus toxoid-containing vaccines (doses) | Clean, minor wound | All other wounds* | ||
|---|---|---|---|---|
| DTaP, Tdap or Td† | TIG‡ | DTaP, Tdap or Td† | TIG‡ | |
| Unknown or <3 | Yes | No | Yes | Yes |
| ≥3 | No§ | No | No¶ | No |
Footnotes
Abbreviations: DTaP = Diphtheria and Tetanus toxoids and acellular pertussis vaccine; Tdap = tetanus toxoid, reduced diphtheria toxoid, and acellular pertussis; Td = tetanus and diphtheria toxoids; TIG = Tetanus immune globulin
*Such as, but not limited to, wounds contaminated with dirt, feces, soil, and saliva; puncture wounds; avulsions; and wounds resulting from missiles, crushing, burns, and frostbite.
† DTaP is recommended for children <7 years of age. Tdap is preferred to Td for persons aged 11 years or older who have not previously received Tdap. Persons aged 7 years or older who are not fully immunized against pertussis, tetanus, or diphtheria should receive one dose of Tdap for wound management and as part of the catch-up series.
‡ People with HIV infection or severe immunodeficiency who have contaminated wounds (including minor wounds) should also receive TIG, regardless of their history of tetanus immunizations.
§ Yes, if ≥10 years since the last tetanus toxoid-containing vaccine dose.
¶ Yes, if ≥5 years since the last tetanus toxoid-containing vaccine dose.
Prevention through Routine Vaccination
Since people cannot naturally acquire immunity to tetanus, the best way to prevent tetanus is to vaccinate your patients. CDC recommends tetanus vaccines for all babies and children, preteens and teens, and adults. See Diphtheria, Tetanus, and Pertussis Vaccination: Information for Healthcare Professionals for information on all tetanus vaccine recommendations by vaccine and age.
References
- Liang JL, Tiwari T, Moro P, et al. Prevention of Pertussis, Tetanus, and Diphtheria with Vaccines in the United States: Recommendations of the Advisory Committee on Immunization Practices (ACIP). MMWR Morb Mortal Wkly Rep. 2018;67(2):1–44.
- American Academy of Pediatrics. Tetanus. In: Kimberlin DW, Brady MT, Jackson MA, Long SS, eds. Red Book®: 2015 Report of the Committee on Infectious Diseases. American Academy of Pediatrics; 2015; 773–8.
- Pink Book’s Chapter on Tetanus
Epidemiology & Prevention of Vaccine-Preventable Diseases
Cholera in Zimbabwe: Current status
Saturday, September 22nd, 2018
On 6 September 2018, a cholera outbreak in Harare was declared by the Ministry of Health and Child Care (MoHCC) of Zimbabwe and notified to WHO on the same day. Twenty-five patients were admitted to a hospital in Harare presenting with diarrhoea and vomiting on 5 September. The first case, a 25-year-old woman, presented to a hospital and died on 5 September. A sample from the woman tested positive for Vibrio cholerae serotype O1 Ogawa. All 25 patients had typical cholera symptoms including excessive vomiting and diarrhoea with rice watery stools and dehydration. The MoHCC declared the outbreak after 11 cases were confirmed for cholera using rapid diagnostic test (RDT) kits and the clinical presentation. Thirty-nine stool samples were collected for culture and sensitivity, 17 of which tested positive for V. cholerae serotype O1 Ogawa.
There has been rapid increase in the number of suspected cases reported per day since 1 September; there was a peak with 473 suspected cases notified on 9 September. As of 15 September 2018, 3621 cumulative suspected cases, including 71 confirmed cases, and 32 deaths have been reported (case fatality ratio: 0.8 %); of these, 98% (3564 cases) were reported from the densely populated capital Harare. The most affected suburbs in Harare are Glen View and Budiriro.
Cases with epidemiological links to cases from Harare have been recently reported from across the country, including in Mashonaland Central Province (Shamva District), Midlands Province (Gokwe North District), Manicaland Province (Buhera and Makoni districts), Masvingo Province and Chitungwiza City.
Public health response
-
- The MoHCC declared the cholera outbreak in Harare City on 6 September; the Government declared the outbreak an emergency and subsequently a disaster on 13 and 14 September, respectively.
- Outbreak coordination committees at the national and district levels have been established.
- WHO and the WHO Country Office (WCO) are supporting the MoHCC with coordination, scaling up the response, strengthening surveillance and mobilizing both national and international health experts to form a cholera surge team.
- WHO experts are providing technical support to laboratories, improving diagnostics and strengthening infection and prevention control (IPC) in communities and health clinics.
- The Government is assessing the potential benefits of conducting an oral cholera vaccine (OCV) campaign; WHO is deploying an expert in OCV campaigns to Harare to support this assessment.
- A cholera treatment centre (CTC) was established by Médecins Sans Frontières (MSF) in Glen View, Harare; MSF has provided extra nurses to support the response.
- The recruitment of additional nurses to strengthen the response is ongoing.
- WHO is providing supplies which contain oral rehydration solution, intravenous fluids and antibiotics for the treatment of patients in CTCs set up by partners.
- Risk communication activities in affected and at-risk districts are being conducted by the Government and health partners.
WHO risk assessment
The outbreak started on 5 September and the number of cases notified per day continues to rapidly increase, particularly in Glen View and Budiriro suburbs of Harare. Cases with epidemiological links to this outbreak have been reported from other provinces across the country. Glen View, which is the epicentre of the outbreak, is an active informal trading area where people come from across the city and the rest of the country to trade. Key risk factors for cholera in Zimbabwe include the deterioration of sanitary and health infrastructure and increasing rural-urban migration which further strains the water and sanitation infrastructure. In Harare, contaminated water from boreholes and wells is suspected to be the source of the outbreak. The water supply situation in Harare remains dire due to the high demand of water that is not being met by the city supply. The country’s available response capacities are overstretched as authorities are already responding to a large typhoid outbreak which started in August 2018. WHO assessed the overall public health risk to be high at the national level and moderate at the regional and low at global levels.
WHO advice
WHO recommends proper and timely case management in CTCs. Increasing access to potable water, improving sanitation infrastructure, and strengthening hygiene and food safety practices in affected communities are the most effective means to prevent and control cholera. Key public health communication messages should be provided to the affected population.
WHO advises against any restrictions on travel or trade to or with Zimbabwe based on the information currently available in relation to this outbreak.
For further information, please refer to: