Archive for April, 2017
4/15/13: Boston Marathon Bombings killing three spectators and wounding more than 260 other people in attendance
Sunday, April 16th, 2017The RMS Titanic, billed as unsinkable, sinks into the icy waters of the North Atlantic after hitting an iceberg on its maiden voyage, killing 1,517 people.
Saturday, April 15th, 2017
Hong Kong’s Centre for Health Protection’s weekly update of H7N9 avian flu in mainland China: 14 new cases, 2 of them fatal.
Saturday, April 15th, 2017The Centre for Health Protection (CHP) of the Department of Health today (April 14) received notification of 14 additional human cases of avian influenza A(H7N9), including two deaths, from the National Health and Family Planning Commission, and strongly urged the public to maintain strict personal, food and environmental hygiene both locally and during travel, particularly in Easter.
The eleven male and three female patients, aged from 39 to 81, had onset from March 27 to April 11, including three from Sichuan, two each from Henan, Shandong and Xizang, and one each from Anhui, Beijing, Hunan, Tianjin and Zhejiang. Among them, 13 had exposure to poultry, poultry markets or mobile stalls.
Travellers to the Mainland or other affected areas must avoid visiting wet markets, live poultry markets or farms. They should be alert to the presence of backyard poultry when visiting relatives and friends. They should also avoid purchase of live or freshly slaughtered poultry, and avoid touching poultry/birds or their droppings. They should strictly observe personal and hand hygiene when visiting any place with live poultry.
Travellers returning from affected areas should consult a doctor promptly if symptoms develop, and inform the doctor of their travel history for prompt diagnosis and treatment of potential diseases. It is essential to tell the doctor if they have seen any live poultry during travel, which may imply possible exposure to contaminated environments. This will enable the doctor to assess the possibility of avian influenza and arrange necessary investigations and appropriate treatment in a timely manner.
While local surveillance, prevention and control measures are in place, the CHP will remain vigilant and work closely with the World Health Organization and relevant health authorities to monitor the latest developments.
The CHP’s Port Health Office conducts health surveillance measures at all boundary control points. Thermal imaging systems are in place for body temperature checks on inbound travellers. Suspected cases will be immediately referred to public hospitals for follow-up.
The display of posters and broadcasting of health messages in departure and arrival halls as health education for travellers is under way. The travel industry and other stakeholders are regularly updated on the latest information.
The public should maintain strict personal, hand, food and environmental hygiene and take heed of the advice below while handling poultry:
- Avoid touching poultry, birds, animals or their droppings;
- When buying live chickens, do not touch them and their droppings. Do not blow at their bottoms. Wash eggs with detergent if soiled with faecal matter and cook and consume them immediately. Always wash hands thoroughly with soap and water after handling chickens and eggs;
- Eggs should be cooked well until the white and yolk become firm. Do not eat raw eggs or dip cooked food into any sauce with raw eggs. Poultry should be cooked thoroughly. If there is pinkish juice running from the cooked poultry or the middle part of its bone is still red, the poultry should be cooked again until fully done;
- Wash hands frequently, especially before touching the mouth, nose or eyes, before handling food or eating, and after going to the toilet, touching public installations or equipment such as escalator handrails, elevator control panels or door knobs, or when hands are dirtied by respiratory secretions after coughing or sneezing; and
- Wear a mask if fever or respiratory symptoms develop, when going to a hospital or clinic, or while taking care of patients with fever or respiratory symptoms.
The public may visit the CHP’s pages for more information: the avian influenza page, the weekly Avian Influenza Report, global statistics and affected areas of avian influenza, the Facebook Page and the YouTube Channel.
Issued at HKT 19:10
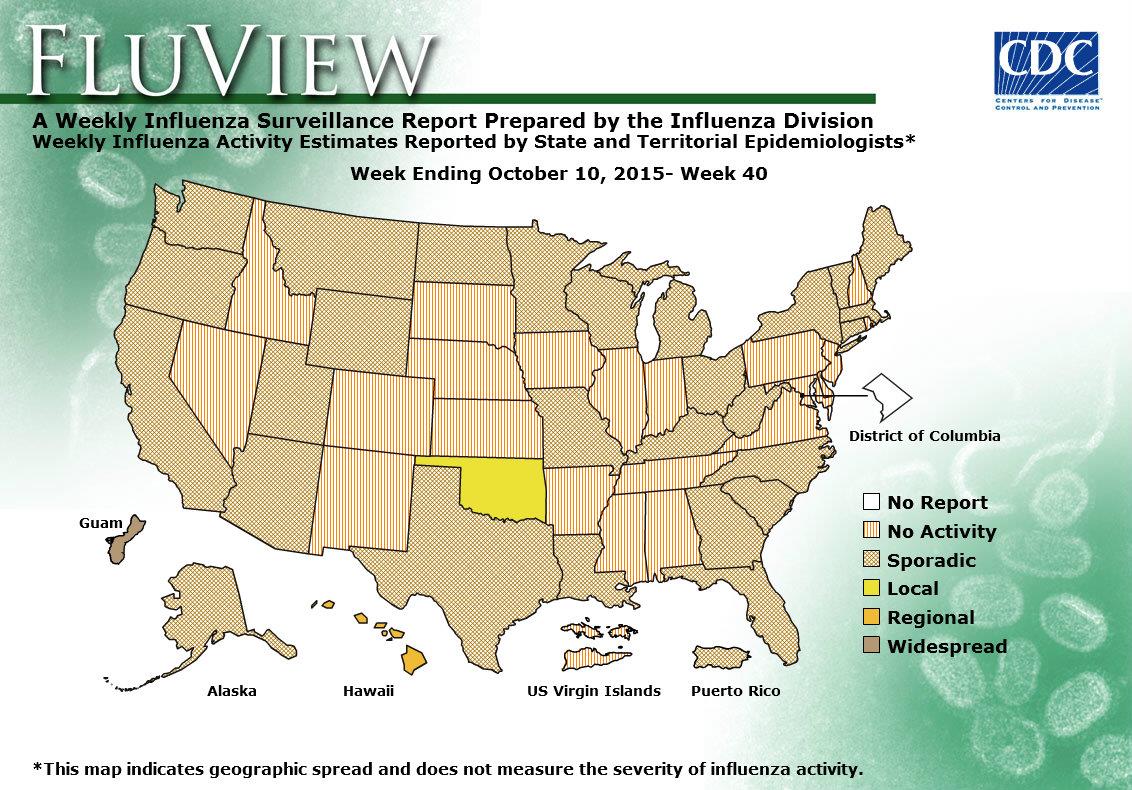
2016-2017 Influenza Season Week 14 ending April 8, 2017
Saturday, April 15th, 2017Synopsis:
During week 14 (April 2-8, 2017), influenza activity decreased but remained elevated in the United States.
- Viral Surveillance: The most frequently identified influenza virus type reported by public health laboratories during week 14 was influenza B. The percentage of respiratory specimens testing positive for influenza in clinical laboratories decreased.
- Pneumonia and Influenza Mortality: The proportion of deaths attributed to pneumonia and influenza (P&I) was below the system-specific epidemic threshold in the National Center for Health Statistics (NCHS) Mortality Surveillance System.
- Influenza-associated Pediatric Deaths: Five influenza-associated pediatric deaths were reported, four that occurred during the 2016-2017 season and one that occurred during the 2010-2011 season.
- Influenza-associated Hospitalizations: A cumulative rate for the season of 59.4 laboratory-confirmed influenza-associated hospitalizations per 100,000 population was reported.
- Outpatient Illness Surveillance: The proportion of outpatient visits for influenza-like illness (ILI) was 2.6%, which is above the national baseline of 2.2%. Five of ten regions reported ILI at or above their region-specific baseline levels. Two states experienced high ILI activity; seven states experienced moderate ILI activity; New York City and 11 states experienced low ILI activity; Puerto Rico and 30 states experienced minimal ILI activity; and the District of Columbia had insufficient data.
- Geographic Spread of Influenza: The geographic spread of influenza in 18 states was reported as widespread; Guam, Puerto Rico, and 18 states reported regional activity; the District of Columbia and 12 states reported local activity; two states reported sporadic activity; and the U.S. Virgin Islands reported no activity.
Texas experiences a 20-year high in mumps cases
Saturday, April 15th, 2017Texas Alerts Providers, Public about Mumps as Cases Reach 20-year High
News Release
April 12, 2017
Cases include spring break travelers to South Padre Island
The Texas Department of State Health Services is advising health care providers to be on alert for mumps in their patients as the state experiences a 20-year high in mumps cases. State, regional and local health departments are currently investigating multiple outbreaks throughout the state, including one involving possible exposures on South Padre Island, a popular spring break destination for students from Texas and elsewhere in the United States. Texas has had 221 mumps cases this year, the largest total since there were 234 cases in 1994.
Mumps cases potentially linked to South Padre Island first came to light this week when another state health department contacted DSHS about a patient with mumps who had traveled to the area for spring break. DSHS alerted other states and has been notified of 13 mumps cases in people who traveled to South Padre Island between March 8 and March 22 from six states, including two cases from Texas.
Mumps symptoms include swollen or tender salivary glands, swollen or tender testicles, low fever, tiredness and muscle aches. People usually develop symptoms 16-18 days after being exposed to the virus, but it can be as long as 25 days. People who think they have mumps should contact their health care provider, and anyone suspected of having mumps should stay home while they’re contagious – five days after swollen glands occur.
Health care providers should consider mumps in patients with compatible symptoms and ask them about travel out of state, to South Padre Island from March 8 to 22 or about any possible exposure to someone with mumps. DSHS also reminds providers they must report suspected mumps cases to their local health department within one work day. Additional information for providers is in the health advisory at http://www.dshs.texas.gov/news/releases/2017/HealthAdvisory-04122017.aspx.
Mumps is highly contagious and is spread through coughing and sneezing and sharing cups and utensils. The mumps vaccine is the best way to keep from getting mumps, and research shows the mumps vaccine protects 88 percent of people who are fully vaccinated. However, some vaccinated people still get sick if they’re exposed to the virus, so it’s also important for people to help stop the spread of mumps by covering coughs and sneezes, washing their hands frequently with soap and water, and not sharing food and drinks. If you don’t know your vaccination status, talk to your health care provider about getting vaccinated.
-30-
Nigeria: Trying to contain an outbreak of meningitis C
Friday, April 14th, 201713 April 2017
A vaccination campaign is underway in Nigeria to contain an outbreak of meningitis C, a strain of meningitis which first emerged in the country in 2013. Since the beginning of this year, the country has reported 4637 suspected cases and 489 deaths across five states.

The International Coordinating Group (ICG) on Vaccine Provision, which coordinates the provision of emergency vaccine supplies during outbreak emergencies, has sent 500 000 doses of meningitis C-containing vaccine to Nigeria to combat the epidemic. The vaccines, funded by Gavi, the Vaccine Alliance, have been administered in Zamfara and Katsina states, which are the worst affected by the outbreak. An additional 820 000 doses of a meningitis C conjugate vaccine – a donation from the UK government to the World Health Organization (WHO) – is being sent to the country.
In the last week, the ICG, which is managed by the International Federation of Red Cross and Red Crescent Societies (IFRC), Médecins sans Frontières (MSF), the United Nations Children’s Fund (UNICEF), and WHO, has also sent 341 000 doses of the Gavi-supported meningitis C-containing vaccine to Niger, where there are over 1300 suspected cases of the disease in districts that border with Nigeria and in the Niamey region of the country.
Meningococcal meningitis is a bacterial form of meningitis, a serious infection of the thin lining that surrounds the brain and spinal cord and can cause severe brain damage. Meningococcal meningitis is fatal in 50% of cases if untreated. Though cases of meningitis occur throughout the world, large, recurring epidemics affect an extensive region of sub-Saharan Africa known as the “meningitis belt” which includes 26 countries from Senegal in the west to Ethiopia in the east.
There are several different types of meningococcal meningitis (A, C, W, etc.) that can cause epidemics. Substantial progress has been made in recent years in protecting Africa from disease due to one of the main epidemic types, through the successful introduction of the Men A conjugate vaccine (MACV) against meningitis A. Since MACV was introduced in 2010, more than 260 million people have been vaccinated across 19 countries. This has resulted in a reduction of the number of meningitis cases by more than 57%. Much work, however, remains to be done to protect the region from meningitis C outbreaks and other types of the disease.
In addition to the use of vaccinations to prevent the transmission of meningitis, 20 000 vials of antibiotics have been sent by the ICG to treat people who have the disease in Nigeria. “Vaccination can drastically reduce the magnitude of the epidemic,” says Dr Sylvie Briand, Director of Infectious Hazard Management for WHO. “But in addition, it is essential to strengthen the care of all those affected by the infection and to ensure those people living in hard-to-reach areas can get treatment.”
The Nigeria Centre for Disease Control, with support from WHO, US CDC, UNICEF and other partners, is leading and coordinating the response to the ongoing outbreak, including intensified surveillance, capacity building for case management and risk communication. WHO’s Country Office in Nigeria, including a number of field offices, have been supporting the government since the outbreak began. An additional team of WHO of meningitis experts has arrived in Nigeria to provide additional epidemic response. “In addition to improving the care of the sick, we are focusing on ensuring accurate information about the spread of the outbreak is available as quickly as possible to help us make the most effective use of vaccines,” says Dr Wondimagegnehu Alemu, WHO Representative to Nigeria.
The emergence of meningitis C in Africa
Since 2013, there have been outbreaks of meningitis C in Nigeria, initially limited to a few areas in Kebbi and Sokoto states in 2013 and 2014. In 2015, however, there were more than 2500 cases of the disease across 3 states in Nigeria as well as 8500 cases in Niger.
Concerns about vaccine supply
Most vaccines currently being used for meningitis C outbreaks in Africa are polysaccharide vaccines, which are in short supply as they are being phased out in other parts of the world. The more effective and long-lasting conjugate vaccines, however, are not readily accessible for outbreak response in the region. The ICG global emergency stockpile currently has approximately 1.2 million doses of meningitis C-containing vaccines left.
“The very limited supply of vaccines to control outbreaks of meningitis C can affect our ability to control these epidemics,” says Dr Olivier Ronveaux, WHO meningitis expert. “In the long term, the accelerated development of affordable and effective conjugate vaccines to cover all epidemic types of meningitis is a high priority for WHO and partners.”
Nigeria and meningitis A
In the past, Nigeria has suffered large-scale outbreaks of meningitis A. In 2009, such an outbreak in the country caused over 55 000 cases with close to 2500 deaths. Niger was also affected, with 13 000 cases and 550 deaths. However, preventive mass vaccination campaigns supported by Gavi and partners, using the safe and effective MACV in Niger (2010-11) and Nigeria (2011-14) have provided high and long-term protection against the bacteria. Since 2010, less than 20 cases of meningitis A have been reported from all vaccinated areas in the region. WHO recommends the continued roll-out of the Men A conjugate vaccine campaigns along with its introduction into routine immunization to prevent a major recurrence of devastating meningitis A epidemics.
President Bashar al-Assad of Syria: Videos of victims, including dead and convulsing children, had been faked.
Thursday, April 13th, 2017CORDS on leishmaniasis
Thursday, April 13th, 2017“…New research out today (9 Feb 2016); the Leishmaniasis Gap Analysis Report and Action Plan carried out in Albania, Jordan and Pakistan during 2015, shows despite its worldwide prevalence and disastrous impact on the lives of millions, leishmaniasis is still very much a growing, neglected disease, mainly affecting impoverished communities, living in poor conditions, without adequate access to shelter, healthcare and medication…..”
“….Leishmaniasis, one of the world’s oldest recorded diseases dating back to the 7th century BC, is an entirely treatable parasitic disease spread by female sandflies. Around 310,000,000 people are estimated to be at risk globally, with around 1.6 million new cases each year across 98 countries. The cutaneous form of the disease can lead to distressing and disfiguring skin ulcers and scarring, while visceral leishmaniasis, which affects organs such as the liver and spleen, is invariably fatal if not treated. Over 40,000 people die from the disease every year, making it the second-largest parasitic killer in the world after malaria.
The purpose of the study is to improve the capacity for the diagnosis, treatment and control of leishmaniasis and other vector borne diseases.
Our research found that;
- leishmaniasis is highly correlated with poverty, malnutrition and other diseases which affect immunity, as well as factors such as crowded living conditions and poor sanitation.
- the real health burden of leishmaniasis remains largely unknown with only 600,000 of the estimated 1.6 million cases each year being diagnosed and treated. This is because those who are most affected are from marginalised communities in rural areas or urban slums, who are unable to seek medical attention because of cost and lack of access to treatment
- in the majority of cases leishmaniasis cannot be transmitted directly from an infected person or animal to another person. Rather it requires the presence of female sandfly vectors to spread the disease. It is not therefore a disease that is likely to spread in areas such as Western Europe, which generally lack sandflies and have healthy populations with good sanitation and access to high-quality healthcare
- leishmaniasis has been ignored largely because of its association with poverty and the limited capacity of governments and aid agencies to deal with its complex epidemiology
- it has also been a low priority for multinational pharmaceutical companies to invest in research to develop effective vaccines and therapies……”
In Ready or Not? Protecting the Public from Diseases, Disasters and Bioterrorism, 26 states and Washington, D.C. scored a six or lower on 10 key indicators of public health preparedness.
Thursday, April 13th, 2017Ready or Not? examines the nation’s ability to respond to public health emergencies, tracks progress and vulnerabilities, and includes a review of state and federal public health preparedness policies. Some key findings include:
- 26 states increased or maintained funding for public health from Fiscal Year (FY) 2014-2015 to FY 2015-2016.
- Just 10 states vaccinated at least half of their population (ages 6 months and older) against the seasonal flu during the 2015-2016 flu season (from July 2015 to May 2016).
- 45 states and Washington, D.C. increased the speed of DNA fingerprinting using pulsed-field gel electrophoresis (PFGE) testing for all reported cases of Shiga toxin-producing E. coli O157, a measure of a state’s ability to detect foodborne outbreaks.
- 10 states have a formal access program or a program in progress for getting private sector healthcare staff and supplies into restricted areas during a disaster.
- 30 states and Washington, D.C. met or exceeded the overall national average score (6.7) of the National Health Security Preparedness Index (as of 2016).
- 32 states and Washington, D.C. received a grade of C or above in States at Risk: America’s Preparedness Report Card, a national assessment of state-level preparedness for climate change-related threats – which have an impact on human health.
In addition, the report examined trends in public health preparedness over the last 15 years, finding successes and ongoing concerns.
- One-third of funds for health security and half of funds for healthcare system preparedness have been cut: Health emergency preparedness funding for states has been cut from $940 million in fiscal year (FY) 2002 to $660 million in FY 2016; and healthcare system preparedness funding for states has been cut by more than half since FY 2005 – down to $255 million.
- Some major areas of accomplishment: Improved emergency operations, communication and coordination; support for the Strategic National Stockpile and the ability to distribute medicines and vaccines during crises; major upgrades in public health labs and foodborne illness detection capabilities; and improvements in legal and liability protections during emergencies.
- Some major ongoing gaps: Lack of a coordinated, interoperable, near real-time biosurveillance system; insufficient support for research and development of new medicines, vaccines and medical equipment to keep pace with modern threats; gaps in the ability of the healthcare system to care for a mass influx of patients during a major outbreak or attack; and cuts to the public health workforce across states.
The Ready or Not? report provides a series of recommendations that address many of the major gaps in emergency health preparedness, including:
- Requiring strong, consistent baseline public health Foundational Capabilities in regions, states and communities-so that everyone is protected.
- Ensuring stable, sufficient health emergency preparedness funding to maintain a standing set of foundational capabilities alongside a complementary Public Health Emergency Fund which would provide immediate surge funding during an emergency.
- Improving federal leadership before, during and after disasters – including at the White House level.
- Recruiting and training a next generation public health workforce with expert scientific abilities to harness and use technological advances along with critical thinking and management skills to serve as the Chief Health Strategist for a community.
- Reconsidering health system preparedness for new threats and mass outbreaks by developingstronger coalitions and partnerships among providers, hospitals, insurance providers, pharmaceutical and health equipment businesses, emergency management, and public health agencies.
- Prioritizing efforts to address one of the most serious threats to human health by expanding efforts to stop Superbugs and antibiotic resistance.
- Improving rates of vaccinations for children and adults – which are one of the most effective public health tools against many infectious diseases.
Ready or Not? was released annually from 2003-2012, and more recently, TFAH has released Outbreaks: Protecting Americans from Infectious Diseases, from 2013-2015.The report was supported by a grant from the Robert Wood Johnson Foundation (RWJF).
Score Summary:
A full list of all of the indicators and scores and the full report are available on TFAH’s website. For the state-by-state scoring, states received one point for achieving an indicator or zero points if they did not achieve the indicator. Zero is the lowest possible overall score, 10 is the highest. The data for the indicators are from publicly available sources or were provided from public officials.
10 out of 10: Massachusetts
9 out of 10: North Carolina and Washington
8 out of 10: California, Connecticut, Iowa, New Jersey, Tennessee and Virginia
7 out of 10: Colorado, Delaware, Florida, Indiana, Maryland, Michigan, New Hampshire, New Mexico, New York, North Dakota, Oregon, Rhode Island, South Carolina, Utah and Wisconsin
6 out of 10: Arizona, Arkansas, District of Columbia, Georgia, Hawaii, Illinois, Kansas, Kentucky, Louisiana, Maine, Minnesota, Mississippi, Montana, Nebraska, Ohio, Pennsylvania, Texas and Vermont
5 out of 10: Alabama, Missouri, Oklahoma, South Dakota and West Virginia
4 out of 10 Nevada and Wyoming
3 out of 10: Alaska and Idaho