Archive for the ‘Candida auris’ Category
C. auris may be the first example of a new fungal disease emerging from climate change
Tuesday, August 6th, 2019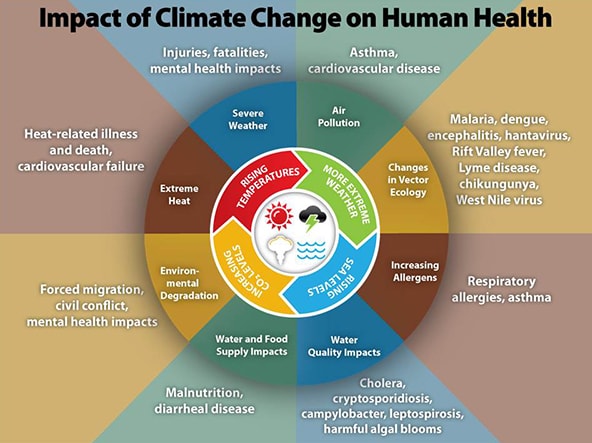
CDC video on Candida auris-2019
Tuesday, August 6th, 2019
Candida auris (C. auris) is an emerging fungus that presents a serious global health threat. CDC is concerned about C. auris for 3 main reasons:
- It is often multidrug-resistant, meaning multiple antifungal drugs are less or not at all effective in treating C. auris.
- It is difficult to identify with standard laboratory methods, and it can be misidentified in labs without specific technology. Misidentification may lead to inappropriate management.
- It has caused outbreaks in healthcare settings. It is important to quickly identify C. auris in a hospitalized patient so that healthcare facilities can take special precautions to stop its spread.
Most C. auris cases in the United States have been detected in the New York City area, New Jersey, and the Chicago area. Clusters of cases have also recently been described in Florida, Texas, and California. C. auris cases in the United States are originally a result of inadvertent introduction into the United States from a patient who had received healthcare in a country where C. auris has been reported. Most cases now are a result of local spread after such an introduction.
The United States now has 340 confirmed cases of Candida auris
Thursday, July 26th, 2018July 23, 2018: Case Count Updated as of June 30, 2018
Candida auris is an emerging fungus that presents a serious global health threat. C. auris causes severe illness in hospitalized patients in several countries, including the United States. Patients can remain colonized with C. auris for a long time and C. auris can persist on surfaces in healthcare environments. This can result in spread of C. auris between patients in healthcare facilities.
Most C. auris cases in the United States have been detected in the New York City area, New Jersey, and the Chicago area. Strains of C. auris in the United States have been linked to other parts of the world. U.S. C. auris cases are a result of inadvertent introduction into the United States from a patient who recently received healthcare in a country where C. auris has been reported or a result of local spread after such an introduction.
Candida auris: From 2013 through 2017 European officials recorded 620 cases, mostly from four large outbreaks, and 110 of them (17.7%) involved bloodstream infections
Saturday, March 31st, 2018C. auris “is an emerging fungus that is causing difficult-to-control outbreaks of invasive healthcare-associated infections. Since the first report of C. auris in 2009 [2], cases have been reported worldwide. Identification of C. auris requires specialised laboratory methodology as traditional identification methods may lead to misidentification [3,4]. In addition, C. auris has been associated with resistance to multiple antifungal classes [5] and difficulties related to the interpretation of antifungal susceptibility results [6]. The combination of these characteristics, i.e. propensity to cause nosocomial outbreaks, multi-drug resistance, ability to cause severe disease and difficulties with laboratory detection, render C. auris a public health threat ….”

There are now 174 cases of Candida auris infections in the United States, 17 more than the CDC reported last month.
Tuesday, December 19th, 2017December 15, 2017: Case Count Updated as of November 30, 2017
Candida auris is an emerging fungus that presents a serious global health threat. C. auris causes severe illness in hospitalized patients in several countries, including the United States. Patients can remain colonized with C. auris for a long time and C. auris can persist on surfaces in healthcare environments. This can result in spread of C. auris between patients in healthcare facilities.
Most C. auris cases in the United States have been detected in the New York City area and New Jersey. Strains of C. auris in the United States have been linked to other parts of the world. U.S. C. auris cases are a result of inadvertent introduction into the United States from a patient who recently received healthcare in a country where C. auris has been reported or a result of local spread after such an introduction.
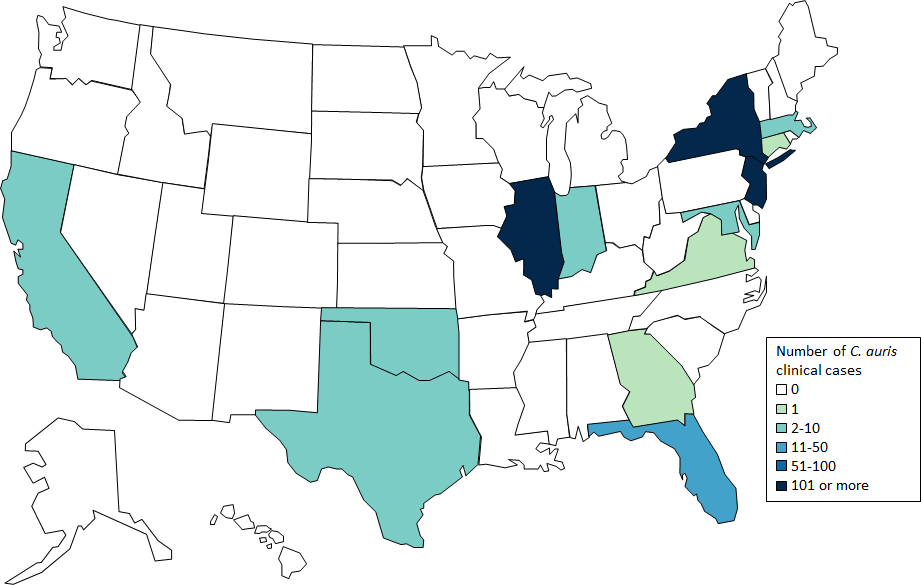
U.S. Map: Clinical cases of Candida auris reported by state, United States, as of November 30, 2017
Cases are categorized by the state where the specimen was collected. Most probable cases were identified when laboratories with current cases of C. auris reviewed past microbiology records for C. auris. Isolates were not available for confirmation. Early detection of C. auris is essential for containing its spread in healthcare facilities.
Table: Clinical cases of Candida auris reported by state, United States, as of November 30, 2017
| State | Number and type of clinical Candida auris cases reported | |
|---|---|---|
| Confirmed | Probable | |
| California | 1 | 0 |
| Connecticut | 1 | 0 |
| Florida | 2 | 0 |
| Illinois | 12 | 2 |
| Indiana | 1 | 0 |
| Maryland | 2 | 0 |
| Massachusetts | 6 | 0 |
| New Jersey | 38 | 23 |
| New York | 110 | 4 |
| Oklahoma | 1 | 0 |
| TOTAL | 174 | 29 |
Beyond the clinical case counts reported above, an additional 257 patients have been found to be colonized with C. auris by targeted screening in four states with clinical cases.
CDC encourages all U.S. laboratories that identify C. auris to notify their state or local public health authorities and CDC at candidaauris@cdc.gov. CDC is working closely with public health and healthcare partners to prevent and respond to C. auris infections. The CDC-sponsored Antibiotic Resistance Laboratory Network (ARLN) will help improve detection and response to C. auris nationwide.
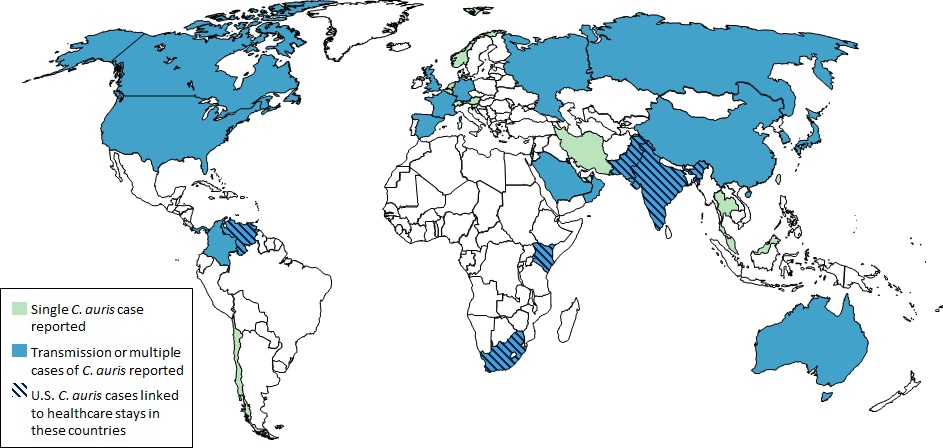
Countries from which Candida auris cases have been reported, as of November 30, 2017
- Single cases of C. auris have been reported from Germany, Japan, Kuwait, and Norway.
- Multiple cases of C. auris have been reported from Canada, Colombia, India, Israel, Kenya, Oman, Pakistan, Panama, South Korea, South Africa, Spain, the United Kingdom, the United States (primarily from New York City Metropolitan Area and New Jersey) and Venezuela; in some of these countries, extensive transmission of C. auris has been documented in more than one hospital.
- U.S. cases of C. auris have been found in patients who had recent stays in healthcare facilities in India, Pakistan, South Africa and Venezuela, which also have documented transmission.
- Other countries not highlighted on this map may also have undetected or unreported C. auris cases.
The United States: 126 confirmed cases of Candida auris as of Aug 31.
Friday, September 22nd, 2017September 18, 2017: Case Count Updated as of August 31, 2017
Candida auris is an emerging fungus that presents a serious global health threat. C. auris causes severe illness in hospitalized patients in several countries, including the United States. Patients can remain colonized with C. auris for a long time and C. auris can persist on surfaces in healthcare environments. This can result in spread of C. auris between patients in healthcare facilities.
Most C. auris cases in the United States have been detected in the New York City area and New Jersey. Strains of C. auris in the United States have been linked to other parts of the world. U.S. C. auris cases are a result of inadvertent introduction into the United States from a patient who recently received healthcare in a country where C. auris has been reported or a result of local spread after such an introduction.
Please note that as of September 18, 2017, the total case counts reported include both probable and confirmed clinical cases; previously reported case counts included only confirmed cases. Case counts for some states are quite a bit higher than those listed before September 18, 2017 because of the change in reporting, and not because of a large increase in new cases. Read more below about how cases are defined.
U.S. Map: Clinical cases of Candida auris reported by state, United States, as of August 31, 2017
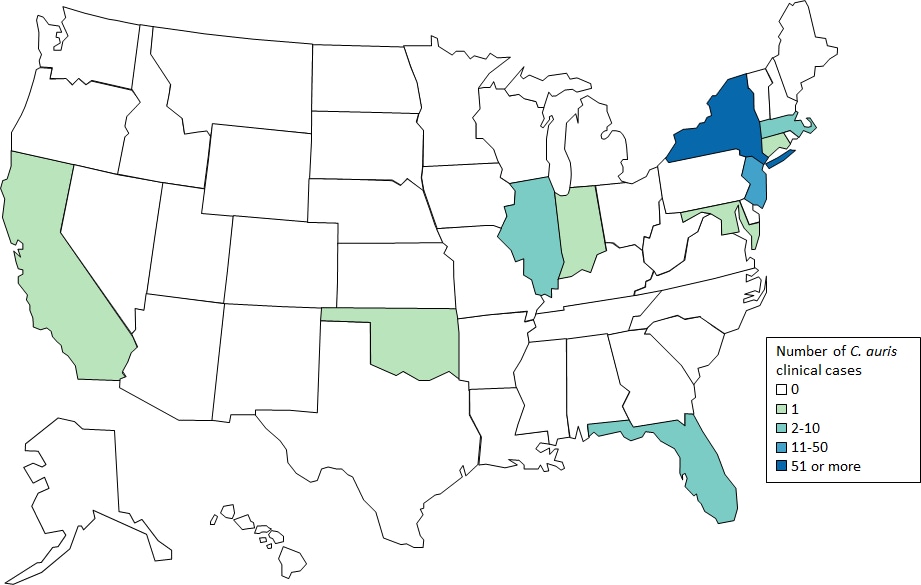 Cases are categorized by the state where the specimen was collected. Most probable cases were identified when laboratories with current cases of C. auris reviewed past microbiology records for C. auris. Isolates were not available for confirmation. Early detection of C. auris is essential for containing its spread in healthcare facilities.
Cases are categorized by the state where the specimen was collected. Most probable cases were identified when laboratories with current cases of C. auris reviewed past microbiology records for C. auris. Isolates were not available for confirmation. Early detection of C. auris is essential for containing its spread in healthcare facilities.
Table: Clinical cases of Candida auris reported by state, United States, as of August 31, 2017
| State | Number and type of clinical Candida auris cases reported | |
|---|---|---|
| Confirmed | Probable | |
| California | 1 | 0 |
| Connecticut | 1 | 0 |
| Florida | 2 | 0 |
| Illinois | 4 | 0 |
| Indiana | 1 | 0 |
| Maryland | 1 | 0 |
| Massachusetts | 3 | 0 |
| New Jersey | 26 | 23 |
| New York | 86 | 4 |
| Oklahoma | 1 | 0 |
| TOTAL | 126 | 27 |
Beyond the clinical case counts reported above, an additional 143 patients have been found to be colonized with C. auris by targeted screening in four states with clinical cases.
CDC will update case counts monthly.
Candida auris is an emerging fungus that presents a serious global health threat.
Wednesday, August 23rd, 2017August 21, 2017: Case Count Updated as of July 31, 2017
What’s New?
- August 21, 2017: case count updated to 112
- July 14, 2017: Updated recommendations on identification(https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html), treatment(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-treatment.html), and infection control(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-infection-control.html)
- June 26, 2017: Fact Sheet on Candida auris(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-drug-resistant.html)
- May 18, 2017: MMWR Notes from the Field on ongoing transmission(https://www.cdc.gov/mmwr/volumes/66/wr/mm6619a7.htm?s_cid=mm6619a7_w%20)
Candida auris is an emerging fungus that presents a serious global health threat. Healthcare facilities in several countries have reported that C. auris has caused severe illness in hospitalized patients. Some strains of C. auris are resistant to all three major classes of antifungal drugs. This type of multidrug resistance has not been seen before in other species of Candida. Also of concern, C. auris can persist on surfaces in healthcare environments and spread between patients in healthcare facilities. CDC has developed identification(https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html), treatment(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-treatment.html), and infection control(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-infection-control.html) recommendations to help prevent the spread of C. auris.
CDC encourages all U.S. laboratory staff who identify C. auris to notify their state or local public health authorities and CDC at candidaauris@cdc.gov.
Candida auris cases in the United States
Location represents the state of C. auris specimen collection. The case counts displayed reflect clinical cases of C. auris (i.e., based on specimens collected in the normal course of care). They do not include patients who screened for presence of C. auris colonization. C. auris has been isolated from an additional 120 patients from healthcare facilities in 4 states where clinical cases were detected. This map will be updated monthly.
Resources
- General Information about Candida auris(https://www.cdc.gov/fungal/diseases/candidiasis/candida-auris-qanda.html)
- Recommendations for Identification(https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html), Treatment(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-treatment.html), and Infection control(https://www.cdc.gov/fungal/diseases/candidiasis/c-auris-infection-control.html) of Candida auris
- June 2016 Clinical Alert: Information for Healthcare Professionals about Candida auris(https://www.cdc.gov/fungal/diseases/candidiasis/candida-auris-alert.html)
- Laboratory Submission Information(https://www.cdc.gov/fungal/lab_submission.html)
Publications
CDC Publications:
- Tsay, S., et. al. Ongoing Transmission of Candida auris in Health Care Facilities — United States, June 2016–May 2017(https://www.cdc.gov/mmwr/volumes/66/wr/mm6619a7.htm). MMWR, 2017, May 18.
- Berkow, et al. In vitro activity of a novel glucan synthase inhibitor, SCY-078, against clinical isolates of Candida auris. Antimicrob Agents Chemother. 2017 May 8.
- Vallabhaneni, S., et. al. Investigation of the first seven reported U.S. cases of Candida auris, a globally-emerging invasive fungus — United States, May 2013–August 2016(https://www.cdc.gov/mmwr/volumes/65/wr/mm6544e1.htm?s_cid=mm6544e1_w) . MMWR, 2016, Nov 4.
- Lockhart, S., et al., Simultaneous emergence of multidrug resistant Candida auris on three continents confirmed by whole genome sequencing and epidemiological analyses. Clinical Infectious Dis, 2016, Oct 20.
Candida auris reported from other countries:
India
- Chowdhary, A., et al., New clonal strain of Candida auris, Delhi, India. Emerg Infect Dis, 2013. 19(10): p. 1670-3.
Israel
- Ben-Ami, R., et al., Multidrug-Resistant Candida haemulonii and C. auris, Tel Aviv, Israel. Emerg Infect Dis, 2017. 23(2): p.195-203.
- Ben-Ami, R., et al., Antibiotic exposure as a risk factor for fluconazole-resistant Candida bloodstream infection. Antimicrob Agents Chemother, 2012. 56(5): p. 2518-23.
Japan
- Satoh, K., et al., Candida auris sp. nov., a novel ascomycetous yeast isolated from the external ear canal of an inpatient in a Japanese hospital. Microbiol Immunol, 2009. 53(1): p. 41-4.
Kuwait
- Emara, M., et al., Candida auris candidemia in Kuwait, 2014. Emerg Infect Dis, 2015. 21(6): p. 1091-2.
South Afria
- Magobo, R.E., et al., Candida auris-associated candidemia, South Africa. Emerg Infect Dis, 2014. 20(7): p. 1250-1.
South Korea
- Choi, et al. Otomastoiditis caused by Candida auris: Case report and literature review. Mycoses. 2017 Apr 5.
- Lee, W.G., et al., First three reported cases of nosocomial fungemia caused by Candida auris. J Clin Microbiol, 2011. 49(9): p. 3139-42.
Spain
- Gaitán, A.C.R., et al. Nosocomial fungemia by Candida auris: First four reported cases in continental Europe. Rev Iberoam Micol, 2017, Jan 25.
United Kingdom
- Borman, A.M., et al. Isolates of the emerging pathogen Candida auris present in the UK have several geographic origins. Med Mycol. 2017 Feb 16.
- Schelenz, S., et al. First hospital outbreak of the globally emerging Candida auris in a European hospital. Antimicrob Resist Infect Control. 2016 Oct 19; 5:35.
Venezuela
- Calvo, B., et al. First report of Candida auris in America: Clinical and microbiological aspects of 18 episodes of candidemia. J Infect, 2016. 73(4): p.369-74.
Recommendations from other countries
- European Centre for Disease Prevention and Control. Candida auris in healthcare settings – Europe – 19 December 2016. Stockholm: ECDC; 2016.
- Candida auris identified in England. Public Health England. 2016, July 1.
- Candida auris: laboratory investigation, management and infection prevention and control. Public Health England. 2016, June 27.
Laboratory aspects of Candida auris
- Larkin, E., et al. The emerging pathogen Candida auris: Growth phenotype, virulence factors, activity of antifungals, and effect of SCY-078, a novel glucan synthesis inhibitor, on growth morphology and biofilm formation. Antimicrob Agents Chemother. 2017 Apr 24;61(5).
- Mizusawa, M., et al. Can a multi-drug resistant Candida auris be reliably identified in clinical microbiology laboratories? J. Clin. Microbiol, 2016, Nov 23.
- Sherry, L., et al., Biofilm-Forming Capability of Highly Virulent, Multidrug-Resistant Candida auris. Emerg Infect Dis, 2017.23(2): p. 328-31.
Other publications
- Azar, M.M., et al. Donor-derived transmission of Candida auris during lung transplantation. Clin Infect Dis. 2017 May 17.
- Clancy, C.J., et al. Emergence of Candida auris: an international call-to-arms. Clinical Infectious Dis, 2016, Oct 20.
Candida auris: 61 cases of the fungus have been reported in the U.S. since 2013
Sunday, May 7th, 2017Candida auris is an emerging fungus that presents a serious global health threat. Healthcare facilities in several countries have reported that C. auris has caused severe illness in hospitalized patients. Some strains of Candida auris are resistant to all three major classes of antifungal drugs. This type of multidrug resistance has not been seen before in other species of Candida. Also of concern, C. auris can persist on surfaces in healthcare environments and spread between patients in healthcare facilities, unlike most other Candida species. CDC has developed Interim Recommendations(https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html) to help prevent the spread of C. auris.

C. auris is difficult to identify with standard laboratory methods and can be misidentified in labs without specific technology. CDC encourages all U.S. laboratory staff who identify C. auris strains to notify their state or local public health authorities and CDC at candidaauris@cdc.gov. Find answers to frequently asked questions about C. auris on our questions and answers page(https://www.cdc.gov/fungal/diseases/candidiasis/candida-auris-qanda.html) and in the Candida auris: Interim Recommendations(https://www.cdc.gov/fungal/diseases/candidiasis/recommendations.html).
CDC is working with state and local health departments to identify and investigate cases of C. auris. The following map displays where C. auris cases have been identified in the United States as of April 13, 2017.