Archive for the ‘Pandemic’ Category
“…..With each fictional pandemic Johns Hopkins experts have designed, the takeaway lesson is the same: We are nowhere near prepared…..”
Monday, December 23rd, 2019“……..That center’s latest pandemic simulation, Event 201, dropped participants right in the midst of an uncontrolled coronavirus outbreak that was spreading like wildfire out of South America to wreak worldwide havoc...…”
Dr. Terrence Tumpey and the Reconstruction of the 1918 Pandemic Virus
Monday, December 23rd, 2019In 2005, microbiologist Dr. Terrence Tumpey was approved by then-CDC director Dr. Julie Gerberding to use reverse genetics to reconstruct the 1918 influenza virus, which had been lost to history following the devastating pandemic of 1918. The decision to recreate the 1918 virus was made very carefully by senior government officials and then carried out under strict controls. Dr. Tumpey was chosen to be the only person authorized to work on the 1918 virus, and then only under biosecurity level 3 enhanced (BSL-3E) precautions. For example, to reduce risk to colleagues, Dr. Tumpey worked alone after normal agency hours. His health was continually monitored and he took influenza antiviral drugs preventively as a precaution in case he was exposed to infectious virus. This remarkable and historic scientific and public health accomplishment was the culmination of years of collaborative work. Using the decoded gene sequence of the 1918 virus obtained by researchers at the Armed Forces Institute of Pathology and plasmids provided by scientists at Mount Sinai, Dr. Tumpey was the first person to physically reconstruct and then study the live and complete 1918 virus in a laboratory setting. Today, Dr. Tumpey is the branch chief of the Influenza Division’s Immunology and Pathogenesis Branch (IPB) at CDC. One hundred years after the 1918 pandemic, I sat down with Dr. Tumpey to talk about his work on the 1918 virus and its significance.
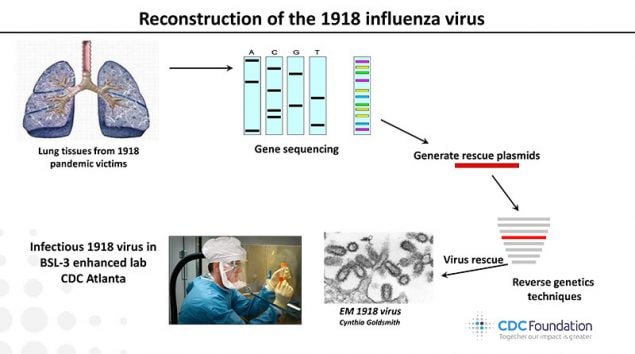
This image shows the order of events leading up to the reconstruction of the 1918 virus by Dr. Terrence Tumpey within CDC’s biosecurity level 3 enhanced laboratory.
Why do you think it’s important to look back on the 1918 pandemic?
Dr. Tumpey: The 1918 influenza pandemic was exceptional as it killed at least 50 million people worldwide, making it the worst influenza pandemic in recent recorded history. Clinicians and scientists of the time were grappling with many unknowns, and what added to the confusion was the erroneous belief that the disease was caused by a bacterium ̶ not a virus ̶ called Pfeiffer’s bacillus (a gram-negative bacterium now recognized as Haemophilus influenzae). It wasn’t for another 30 years that people would understand that the 1918 pandemic virus that infected 30% of the world’s population was an influenza A (H1N1) virus. Because of its impact, the 1918 pandemic is sometimes referred to as the “Mother of all Pandemics,” and it continues to inspire research on its origins and the relationship between the 1918 virus and other influenza viruses.
How or why do you think the 1918 pandemic is still relevant today?
Dr. Tumpey: Understanding the unique features of the 1918 pandemic is especially relevant, as nearly a century later, a descendent of this virus emerged to cause another pandemic. Reports of a novel swine-origin H1N1 virus (2009 H1N1) causing influenza-like illness, pneumonia, and death in people were first announced in April 2009. Laboratory-confirmed cases of human infection rose rapidly as the virus spread. A pandemic was declared on June 11, 2009, at which time 74 countries had reported more than 28,000 human infections with 144 deaths. That virus has continued to circulate as a human seasonal influenza virus since the 2009 pandemic.
How did you become interested in flu as a career path?
Dr. Tumpey: I became very interested in influenza during my graduate studies at the University of South Alabama Medical School. The study of influenza was part of my graduate coursework, and I was always shocked by the exceptionally high mortality rate of the 1918 influenza pandemic. Moreover, in lecturing about the ability of some influenza viruses to spread efficiently between people, one professor gave the example of three people sitting in a room; one has HIV, one has Ebola, and the other is infected with a human influenza virus. If you spend time with those three people in the room (with no contact), which virus will make you sick? That example also got me interested in influenza and influenza transmission. I applied for an American Society of Microbiology (ASM) postdoctoral fellowship with Dr. Jacqueline Katz and received a two-year fellowship to work at CDC’s Influenza Branch and never looked back.
What is the most rewarding part of your work?
Dr. Tumpey: In general, I feel very fortunate to have had the opportunity to study the 1918 virus and other influenza viruses. I particularly enjoy the process of scientific discovery and mentoring trainees in the laboratory. The reconstruction of the 1918 virus also allowed us to study its individual genes and determine why the H1N1 pandemic virus was so lethal. The 1918 virus work revealed a prominent role for the polymerase proteins in enhanced virulence, which resulted in scientists generating new ideas for improving the development of novel antiviral drugs directed against these viral polymerases. As a result, it has been rewarding to see the development of and clinical trials associated with these novel antivirals. These new medications represent an important development as they can potentially expand our available tools against influenza disease.
What are some of the highlights of your research and career?
Dr. Tumpey: I am particularly proud of the characterization of the reconstructed 1918 pandemic virus and subsequent work studying that virus which killed so many. The work, as reported in the October 2005 issue of Science (vol. 310, p 77.)External, was done using a technique called reverse genetics to re-create a living 1918 virus.
How did recreating the 1918 virus make you feel?
I was very excited, and I was very anxious in 2005. When you’re getting ready to remake a virus that is estimated to have killed at least 50 million people worldwide, I was passionate about the great task ahead. I was very fortunate to have the support of CDC and NIH. Before the experiments began, the CDC Office of the Director provided oversight and guidance for this important project. In particular, they carefully evaluated the specific studies to be conducted and concluded that this research could safely and securely be done under BSL-3-enhanced containment. It was decided that I would be the only scientist to rescue the 1918 virus at CDC and I was required to take additional safety precautions that included taking influenza antiviral prophylaxis. In addition, procedures were in place, such that if I experienced influenza-like illness I would quarantine myself at home and avoid contact with the outside world.
Scientifically, everything was in place to be able to remake 1918 influenza virus using a technique called reverse genetics. I was thrilled to be the first person to fully rescue the 1918 virus in the summer of 2005. During multiple weeks in July 2005, my collaborators repeatedly asked me, “Do you have it?” “Has the 1918 virus appeared in culture yet?” When the 1918 virus finally appeared in my BSL-3E cell culture and I knew I had the historic virus in hand, I simply sent an email to my collaborators that read, “That’s one small step for man, one giant leap for mankind.” They knew from the playful email that the 1918 virus was rescued. Overall, the virus rescue was very rewarding and it allowed the 1918 pandemic research to move forward and provide the scientific field with innovative discoveries. In particular, the identification of novel influenza viral factors and new ideas for improving the development of antiviral drugs against all influenza viruses has been gratifying and exciting to watch.
Why was it so important to study the 1918 virus?
Dr. Tumpey: Because the coding sequences of the 1918 viral RNA segments did not reveal obvious genetic features that had been associated with virulence, so it was important to study 1918 recombinant viruses to better understand the genetic markers responsible for virus replication and virulence of this pandemic strain. Thus, I felt like the molecular characterization of the reconstructed 1918 pandemic influenza virus shed light on why this virus was such a killer.
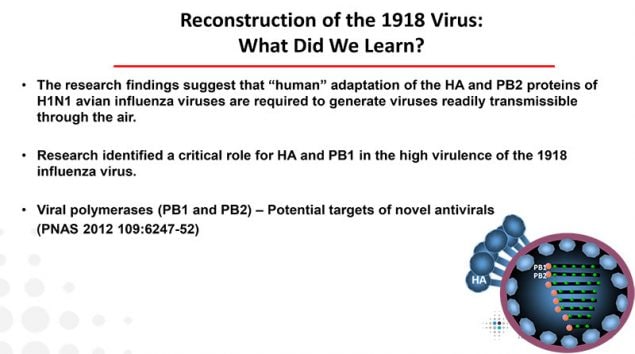
This image lists lessons learned from the study of the reconstructed 1918 virus at CDC and why it was so deadly.
What did you learn about why the 1918 pandemic virus was so deadly?
Dr. Tumpey: We found that the HA and PB1 virus genes of the 1918 virus are essential for maximal replication and virulence. With these data in hand, some scientists felt that these virus genes could be a potential target for a new generation of anti-influenza A drug development. We feel that the quality of the 1918 virus work and end result of the project was remarkable.
How do laboratory safety precautions factor into your job and that of your branch?
Dr. Tumpey: It is increasingly important that staff adhere to biosafety and biosecurity requirements. I am a Select Agent principal investigator (PI), and as PI, I am responsible for full compliance with the policies, practices and procedures put forward by the Select Agent program and Office of the Associated Director of Laboratory Science and Safety (OADLSS). Actually, this important responsibility extends to all aspects of biological safety involving the laboratory environment and all people who enter the BSL-3E space.
What role did you play during the 2009 H1N1 pandemic?
Dr. Tumpey: My role during the 2009 H1N1 pandemic was to perform laboratory experiments with 2009 H1N1 influenza viruses to see how well the virus spread and how severe it was as well as to help evaluate immunity to this novel virus. This helped us assess the potential harm this virus could cause. This was important since the full clinical spectrum of disease caused by 2009 H1N1 influenza viruses and their transmissibility were not completely understood. CDC’s Influenza Division was the first to show that in contrast to seasonal influenza viruses, 2009 H1N1 influenza viruses caused increased morbidity, replicated to higher titers in lung tissue, and were recovered from the intestinal tract of intranasally inoculated ferrets. Interestingly, we found similarities between the 2009 pandemic H1N1 virus and the 1918 H1N1 virus. This was based on several serological studies of the 2009 H1N1 viruses that provided evidence for the presence of cross-reactive antibodies to the 1918 H1N1 virus. Using this information, we demonstrated that vaccination with the seasonal 2010-2011 vaccine (containing the 2009 H1N1 virus) induced neutralizing antibodies to the 1918 virus and protected ferrets against 1918 influenza virus infection. This was a simple study that showed that the seasonal inactivated influenza vaccine that most of us receive would provide protection against the reconstructed 1918 virus which, as a select agent, is considered to pose both biosafety and biosecurity threats.
Do you have any final thoughts on how the lessons learned from your research can help us prepare for the next pandemic?
Taken together, influenza vaccines and antiviral drugs represent critical tools to reduce the burden of influenza virus infection, and they feature prominently in pandemic preparedness and response frameworks. Through the identification of which 1918 virus genes are important for morbidity and the development of vaccines and antivirals, it is clear that reconstruction of the 1918 virus has provided invaluable information towards pandemic preparedness efforts.
Thank you for your time, Dr. Tumpey!
This concludes our CDC expert interview. For more information on Dr. Tumpey’s work and the 100-year anniversary of the 1918 pandemic, please see Dr. Tumpey’s Flu Fighter profile article and CDC’s 1918 pandemic commemoration page.
“According to a new U.S. Army report, Americans could face a horrifically grim future from climate change involving blackouts, disease, thirst, starvation and war. The study found that the US military itself might also collapse. This could all happen over the next two decades…..”
Thursday, October 31st, 2019“…….The report, titled Implications of Climate Change for the U.S. Army, was launched by the U.S. Army War College in partnership with NASA in May at the Wilson Center in Washington DC. The report was commissioned by Gen. Milley during his previous role as the Army’s Chief of Staff……..


The two most prominent scenarios in the report focus on the risk of a collapse of the power grid within “the next 20 years,” and the danger of disease epidemics. Both could be triggered by climate change in the near-term………
The report also warns that the US military should prepare for new foreign interventions in Syria-style conflicts, triggered due to climate-related impacts. Bangladesh in particular is highlighted as the most vulnerable country to climate collapse in the world…..
“The permanent displacement of a large portion of the population of Bangladesh would be a regional catastrophe with the potential to increase global instability,” the report warns. “This is a potential result of climate change complications in just one country. Globally, over 600 million people live at sea level.”
Sea level rise, which could go higher than 2 meters by 2100 according to one recent study, “will displace tens (if not hundreds) of millions of people, creating massive, enduring instability,” the report adds……..“


A World At Risk: Latest scientific report out of the WHO
Saturday, October 26th, 2019“No country is fully equipped to deal with the next global pandemic,…….
Scientists say an outbreak of a flu-like illness could sweep across the planet in 36 hours and kill tens of millions due to our constantly-travelling population.
But a review of health care systems already in place across the world found just 13 countries had the resources to put up a fight against an ‘inevitable’ pandemic…….”
J-IDEA, the Abdul Latif Jameel Institute for Disease and Emergency Analytics will rapidly respond to emergencies such as epidemics, extreme climate events, and natural and humanitarian disasters.
Tuesday, October 22nd, 2019“…..J-IDEA will tackle crises, such as Ebola and MERS, alongside longer-term global priorities, including the impact of climate change on health, using cutting-edge data science and public health research to deliver policy insights.
The new institute brings together the world’s foremost epidemiologists, biostatisticians, medics and data scientists as they break down barriers between academic expertise and on-the-ground impact. ….”
“……J-IDEA brings together over 200 researchers working on global health within Imperial College’s School of Public Health. Partnering with governments and international institutions, J-IDEA advances methods and real-world application of data analytics to identify and support effective actions and high priority investments into population health globally – both in responding to crises but also in identifying the cross-cutting investments which will build strong and resilient health systems better able to meet future health challenges and threats…..”
New Zealand, Australia and Iceland could act as island refuges to save humanity from extinction in the event of a catastrophic global pandemic and researchers have ranked 20 island nations which could act as refuges from which large-scale technological society could be rebuilt.
Monday, October 7th, 2019“……The researchers say that for such a strategy to succeed, preparations must be made ahead of time. They suggest that New Zealand consider investing in resiliency measures and rehearse the rapid introduction of border controls...…”

In the journal:
Risk Analysis DOI: 10.1111/risa.13398
The Prioritization of Island Nations as Refuges from Extreme Pandemics
Matt Boyd and Nick Wilson
Abstract: “In this conceptual article with illustrative data, we suggest that it is useful to rank island na-
tions as potential refuges for ensuring long-term human survival in the face of catastrophic
pandemics (or other relevant existential threats). Prioritization could identify the several is-
land nations that are most suitable for targeting social and political preparations and further
investment in resiliency. We outline a prioritization methodology and as an initial demon-
stration, we then provide example rankings by considering 20 sovereign island states (all with
populations greater than 250,000 and no land borders). Results describe each nation in nine
resilience-relevant domains covering location, population, resources, and society according
to published data. The results indicate that the most suitable island nations for refuge status
are Australia, followed closely by New Zealand, and then Iceland, with other nations all well
behind (including the relatively high-income ones of Malta and Japan). Nevertheless, some
key contextual factors remain relatively unexplored. These include the capacity of the juris-
diction to rapidly close its borders when the emerging threat was first detected elsewhere,
and whether or not large subnational islands should be the preferred focus for refuge design
(e.g., the Australian state of Tasmania, the island of Hokkaido in Japan, or the South Island
of New Zealand). Overall, this work provides conceptual thinking with some initial exam-
ple analysis. Further research could refine the selection of metrics, how best to weight the
relevant domains, and how the populations of prioritized island nations view their nation’s
selection as a potential refuge for human survival.”
AUSTRALIA
NEW ZEALAND
ICELAND
MALTA
JAPAN
CAPE VERDE
BAHAMAS
TRINIDAD/TOBAGO
BARBADOS
MADAGASCAR
CUBA
MAURITIUS
FIJI
MALDIVES
SRI LANKA
COMOROS
SOLOMON ISLANDS
JAMAICA
PHILIPPINES
VANUATU
Quack pharmacists around the world are fueling future superbug pandemics
Tuesday, September 24th, 2019Bureau of Investigative Journalism
“……Despite recent attempts by the Cambodian government to crack down on illegal pharmacies, these sellers fly under the radar. Most do not have any qualifications that would allow them to prescribe the cocktail of drugs they give patients, the researchers from the London School of Hygiene and Tropical Medicine and the University of Health Sciences found.
The invisible sellers had many misconceptions about antibiotics and dispensed them incorrectly, researchers said. Most openly admitted they sold them in response to patients’ demands, rather than medical need, leading to overprescription. They believed that antibiotics were necessary for colds and diarrhoea, and sold short courses of the drugs. They also sold antibiotics designed for humans to people wanting to give them to their cattle, chickens and dogs.
One seller said she learned about medicines during the Khmer Rouge regime and incorrectly believed antibiotics should be smeared into wounds. She said: “We break them into small pieces and pour them on wounds on our legs.”
This kind of misuse speeds up the creation of drug resistant bacteria, or superbugs, which are predicted to kill 10 million people by 2050 if no action is taken…..”
Rubbing hands with ethanol-based sanitizers may not be effective hand hygiene after all.
Friday, September 20th, 2019“……the researchers from the Kyoto Profectural University of Medicine found that ethanol-based disinfectants, or hand sanitizers, would have be in contact for at least 4 minutes with the influenza A virus before killing it, a much longer duration than typical use. After 2 minutes of use, the virus was still active...….”
Project BioShield over 15 years of progress
Saturday, August 17th, 2019ASPR
Project BioShield Evolution: Fifteen Years of Bridging the ‘Valley of Death’ in the Medical Countermeasures Pipeline
Author: By Dr. Robert Kadlec, Assistant Secretary for Preparedness and Response
Published Date: 7/17/2019 12:15:00 PM
Category: Innovations; Medical Countermeasures; National Health Security;
Saving lives in a public health emergency requires cutting-edge medical countermeasures: medications, vaccines, diagnostics, and more. In some types of emergencies, like an act of bioterrorism, some of those medical products have no commercial market. People don’t use an anthrax antitoxin every day – thank goodness. Yet that lack of commercial market also means pharmaceutical or biotech companies had only one possible buyer for their products: the federal government for stockpiling.
In 2004, Congress passed the Project BioShield Act to create a market for products necessary for disaster response but with limited or no commercial market. The Act provides HHS with a multi-year special reserve fund to support late-stage development and manufacturing, and the financial resources to buy these life-saving medical products for the American people to use in public health emergencies. In this way, Project BioShield is a critical part of the U.S. strategy for biodefense and our commitment to the American people.
Last month, Congress took action to further strengthen Project BioShield as part of the Pandemic and All-Hazards Preparedness and Advancing Innovation Act of 2019 (PAHPAIA). PAHPAIA increases the budget authorization and provides ten-year funding for product development. We know next-generation medical countermeasures aren’t developed overnight – in fact, getting a product across the finish line takes many years. Multi-year funding helps BARDA continue building the strong public-private partnerships needed to spur innovation and provide the private sector with the stability needed to produce potentially lifesaving medical countermeasures.
For example, smallpox is one of the most consequential infectious diseases in human history, responsible for nearly 300 million deaths in the 20th century alone. It is also a high-priority threat requiring federal agencies to develop strategies and countermeasures against this threat. Thanks to our partners at NIAID and DoD and the support of Project BioShield, last year our industry partner was issued an FDA approval for a treatment for smallpox via the animal rule. At present, there are now over 2 million treatment courses in ASPR’s Strategic National Stockpile to protect Americans in the event of a smallpox national security emergency.
However, we have found over the past 15 years the most practical and cost-effective approach is, whenever possible, to look at products that not only can be used for emergencies, but also have uses in daily medical care, such as burn care, the radiation effects cancer patients encounter, or seizures.
In some cases, we’ve worked with companies to expand indications for existing products. For example, three medical countermeasures are now FDA-approved to treat patients suffering bone marrow and blood cell damage from acute radiation syndrome. All three of these products were already licensed drugs used to treat patients undergoing radiation therapy for cancer. Project BioShield funding was used to conduct the critical studies needed to expand the indications for these products so they could also be used to treat the damage caused by acute radiation syndrome in a radiation emergency. Using such drugs is helpful in emergencies because healthcare facilities already stock the drugs, and clinicians are already familiar with using them.
We are using Project BioShield to support other new products with commercial market potential. For example, we supported a large study of a seizure treatment because seizures are one of the potentially deadly effects of nerve agents. The product is used commonly in preparing patients for surgery and for epileptic seizures; thanks to Project BioShield, the product is now approved as an antiseizure medication for status epilepticus and has been added to the Strategic National Stockpile for use in a chemical emergency response.
For 15 years, BARDA has been proud to partner with industry to develop cutting-edge medical countermeasures. Our country is better prepared to respond to health security threats because of Project BioShield. We look forward continued collaboration as we work to develop and produce medical countermeasures that can be used to save lives in the event of an emergency.
Baloxavir showed broad-spectrum in vitro replication inhibition of 4 types of influenza viruses
Wednesday, July 10th, 2019Mishin VP, Patel MC, Chesnokov A, De La Cruz J, Nguyen HT, Lollis L, et al. Susceptibility of influenza A, B, C, and D viruses to baloxavir. Emerg Infect Dis. 2019 Oct [date cited]. https://doi.org/10.3201/eid2510.190607
“…….Baloxavir displayed broad antiviral activity against diverse influenza viruses, including all 4 types and animal-origin influenza A viruses with pandemic potential. Our findings suggest that baloxavir might offer the first therapeutic option against influenza C virus infections. Further studies are needed to provide comprehensive assessment of baloxavir susceptibility by using a large panel of representative influenza C viruses. Ongoing monitoring of baloxavir susceptibility of emerging avian and swine influenza A viruses with pandemic potential is needed to inform clinical management and public health preparedness efforts...…”
