Archive for December, 2015
Initial Costs of the 45 Ebola Treatment Centers in the US: $1,197,993 average (total: $53,909,701)
Thursday, December 3rd, 2015Volume 22, Number 2—February 2016
Letter
Initial Costs of Ebola Treatment Centers in the United States
Main Article(http://wwwnc.cdc.gov/eid/article/22/2/15-1431_article)
Table
Initial costs in US$ incurred by 45 Ebola treatment centers in the United States*
| Cost scale | Total costs | Construction/ facility modifications | PPE supplies | Staff training | Unit planning | Laboratory equipment | Non-PPE and nonlaboratory supplies and equipment |
|---|---|---|---|---|---|---|---|
| Average | 1,197,993 | 420,502 | 213,347 | 267,075 | 176,713 | 99,106 | 172,581 |
| Median | 1,000,000 | 202,980 | 110,000 | 150,000 | 82,000 | 84,000 | 100,000 |
| High | 6,556,457 | 3,839,000 | 1,067,573 | 1,624,639 | 1,200,000 | 317,406 | 560,000 |
| Low | 51,500 | 8,500 | 10,000 | 10,000 | 15,000 | 0 | 3,000 |
| Sums† | 53,909,701 | 16,820,080 | 8,747,240 | 10,950,072 | 4,947,966 | 3,865,124 | 6,385,513 |
*PPE, personal protective equipment.
†Summarized data were collected through self-report by individual treatment centers through an electronically administered survey.
Ebola update: •No confirmed cases were reported in the week to 29 November
Thursday, December 3rd, 2015- No confirmed cases were reported in the week to 29 November. Investigations are ongoing into the origin of infection of the cluster of 3 confirmed cases of Ebola virus disease (EVD) reported from Liberia in the week to 22 November. The first-reported case in that cluster was a 15-year-old boy who tested positive for EVD after admission to a health facility in the Greater Monrovia area on 19 November. He was then transferred to an Ebola treatment centre along with the 5 other members of his family. Two other members of the family – the boy’s 8-year old brother and his 40-year-old father – subsequently tested positive for EVD whilst in isolation. The 15-year-old boy died on 23 November. In addition to the family of the first-reported case, 165 contacts have been identified so far, including 34 high-risk contacts. Liberia was previously declared free of Ebola transmission on 3 September 2015.
- On 7 November WHO declared that Sierra Leone had achieved objective 1 of the phase 3 framework, and the country has now entered a 90-day period of enhanced surveillance scheduled to conclude on 5 February 2016. As of 29 November it had been 13 days since the last EVD patient in Guinea received a second consecutive EVD-negative blood test. The last case in Guinea was reported on 29 October 2015.
- The recent cases in Liberia underscore the importance of robust surveillance measures to ensure the rapid detection of any reintroduction or re-emergence of EVD in currently unaffected areas. In order to achieve objective 2 of the phase 3 response framework – to manage and respond to the consequences of residual Ebola risks – Guinea, Liberia, and Sierra Leone have each put surveillance systems in place to enable health workers and members of the public to report any case of illness or death that they suspect may be related to EVD to the relevant authorities. In the week to 29 November, 18 014 such alerts were reported in Guinea, with alerts reported from all of the country’s 34 prefectures. Equivalent data are not currently available for Liberia. In Sierra Leone, 1420 alerts were reported from all 14 districts in the week ending 15 November (the most recent week for which data are available).
- As part of each country’s EVD surveillance strategy, blood samples or oral swabs should be collected from any live or deceased individuals who have or had clinical symptoms compatible with EVD. In the week to 29 November, 8 operational laboratories in Guinea tested a total of 631 new and repeat samples from 15 of the country’s 34 prefectures. 82% of all samples tested in Guinea were swabs collected from dead bodies. By contrast, 84% of the 981 new and repeat samples tested in Liberia over the same period were blood samples collected from live patients. In addition, all 15 counties in Liberia submitted samples for testing by the country’s 5 operational laboratories. 1344 new samples were collected from all 14 districts in Sierra Leone and tested by 8 operational laboratories. 89% of samples in Sierra Leone were swabs collected from dead bodies.
- 994 deaths in the community were reported from Guinea in the week to 29 November through the country’s alerts system. This represents approximately 44% of the 2248 community deaths expected based on estimates of the population and a crude mortality rate of 11 deaths per 1000 people per year. Equivalent data are not yet available for Liberia. In Sierra Leone, 1282 reports of community deaths were received through the alert system during the week ending 15 November (the most recent week for which data are available), representing approximately 62% of the 2075 deaths expected each week based on estimates of the population and a crude mortality rate of 17 deaths per 1000 people per year.
- No confirmed cases were reported in the week to 29 November. Investigations are ongoing into the origin of infection of the cluster of 3 confirmed cases of Ebola virus disease (EVD) reported from Liberia in the week to 22 November. The first-reported case in that cluster was a 15-year-old boy who tested positive for EVD after admission to a health facility in the Greater Monrovia area on 19 November. He was then transferred to an Ebola treatment centre along with the 5 other members of his family. Two other members of the family – the boy’s 8-year old brother and his 40-year-old father – subsequently tested positive for EVD whilst in isolation. The 15-year-old boy died on 23 November. In addition to the family of the first-reported case, 165 contacts have been identified so far, including 34 high-risk contacts. Liberia was previously declared free of Ebola transmission on 3 September 2015.
- On 7 November WHO declared that Sierra Leone had achieved objective 1 of the phase 3 framework, and the country has now entered a 90-day period of enhanced surveillance scheduled to conclude on 5 February 2016. As of 29 November it had been 13 days since the last EVD patient in Guinea received a second consecutive EVD-negative blood test. The last case in Guinea was reported on 29 October 2015.
- The recent cases in Liberia underscore the importance of robust surveillance measures to ensure the rapid detection of any reintroduction or re-emergence of EVD in currently unaffected areas. In order to achieve objective 2 of the phase 3 response framework – to manage and respond to the consequences of residual Ebola risks – Guinea, Liberia, and Sierra Leone have each put surveillance systems in place to enable health workers and members of the public to report any case of illness or death that they suspect may be related to EVD to the relevant authorities. In the week to 29 November, 18 014 such alerts were reported in Guinea, with alerts reported from all of the country’s 34 prefectures. Equivalent data are not currently available for Liberia. In Sierra Leone, 1420 alerts were reported from all 14 districts in the week ending 15 November (the most recent week for which data are available).
- As part of each country’s EVD surveillance strategy, blood samples or oral swabs should be collected from any live or deceased individuals who have or had clinical symptoms compatible with EVD. In the week to 29 November, 8 operational laboratories in Guinea tested a total of 631 new and repeat samples from 15 of the country’s 34 prefectures. 82% of all samples tested in Guinea were swabs collected from dead bodies. By contrast, 84% of the 981 new and repeat samples tested in Liberia over the same period were blood samples collected from live patients. In addition, all 15 counties in Liberia submitted samples for testing by the country’s 5 operational laboratories. 1344 new samples were collected from all 14 districts in Sierra Leone and tested by 8 operational laboratories. 89% of samples in Sierra Leone were swabs collected from dead bodies.
- 994 deaths in the community were reported from Guinea in the week to 29 November through the country’s alerts system. This represents approximately 44% of the 2248 community deaths expected based on estimates of the population and a crude mortality rate of 11 deaths per 1000 people per year. Equivalent data are not yet available for Liberia. In Sierra Leone, 1282 reports of community deaths were received through the alert system during the week ending 15 November (the most recent week for which data are available), representing approximately 62% of the 2075 deaths expected each week based on estimates of the population and a crude mortality rate of 17 deaths per 1000 people per year.
- No confirmed cases were reported in the week to 29 November. Investigations are ongoing into the origin of infection of the cluster of 3 confirmed cases of Ebola virus disease (EVD) reported from Liberia in the week to 22 November. The first-reported case in that cluster was a 15-year-old boy who tested positive for EVD after admission to a health facility in the Greater Monrovia area on 19 November. He was then transferred to an Ebola treatment centre along with the 5 other members of his family. Two other members of the family – the boy’s 8-year old brother and his 40-year-old father – subsequently tested positive for EVD whilst in isolation. The 15-year-old boy died on 23 November. In addition to the family of the first-reported case, 165 contacts have been identified so far, including 34 high-risk contacts. Liberia was previously declared free of Ebola transmission on 3 September 2015.
- On 7 November WHO declared that Sierra Leone had achieved objective 1 of the phase 3 framework, and the country has now entered a 90-day period of enhanced surveillance scheduled to conclude on 5 February 2016. As of 29 November it had been 13 days since the last EVD patient in Guinea received a second consecutive EVD-negative blood test. The last case in Guinea was reported on 29 October 2015.
- The recent cases in Liberia underscore the importance of robust surveillance measures to ensure the rapid detection of any reintroduction or re-emergence of EVD in currently unaffected areas. In order to achieve objective 2 of the phase 3 response framework – to manage and respond to the consequences of residual Ebola risks – Guinea, Liberia, and Sierra Leone have each put surveillance systems in place to enable health workers and members of the public to report any case of illness or death that they suspect may be related to EVD to the relevant authorities. In the week to 29 November, 18 014 such alerts were reported in Guinea, with alerts reported from all of the country’s 34 prefectures. Equivalent data are not currently available for Liberia. In Sierra Leone, 1420 alerts were reported from all 14 districts in the week ending 15 November (the most recent week for which data are available).
- As part of each country’s EVD surveillance strategy, blood samples or oral swabs should be collected from any live or deceased individuals who have or had clinical symptoms compatible with EVD. In the week to 29 November, 8 operational laboratories in Guinea tested a total of 631 new and repeat samples from 15 of the country’s 34 prefectures. 82% of all samples tested in Guinea were swabs collected from dead bodies. By contrast, 84% of the 981 new and repeat samples tested in Liberia over the same period were blood samples collected from live patients. In addition, all 15 counties in Liberia submitted samples for testing by the country’s 5 operational laboratories. 1344 new samples were collected from all 14 districts in Sierra Leone and tested by 8 operational laboratories. 89% of samples in Sierra Leone were swabs collected from dead bodies.
- 994 deaths in the community were reported from Guinea in the week to 29 November through the country’s alerts system. This represents approximately 44% of the 2248 community deaths expected based on estimates of the population and a crude mortality rate of 11 deaths per 1000 people per year. Equivalent data are not yet available for Liberia. In Sierra Leone, 1282 reports of community deaths were received through the alert system during the week ending 15 November (the most recent week for which data are available), representing approximately 62% of the 2075 deaths expected each week based on estimates of the population and a crude mortality rate of 17 deaths per 1000 people per year.
PAHO issues an alert about the Zika virus threat, urging countries in the region to be on the lookout for the disease and to watch for unusual patterns in newborns.
Thursday, December 3rd, 2015** There has been an unusual rise in microcephaly in Brazil’s hardest hit Zika virus regions
** Brazil’s health ministry is reporting a twentyfold increase in microcephaly cases compared to previous years.
** 1,248 cases reported in Brazil.
** French Polynesian health authorities have also reported an unusual increase in central nervous system malformations in babies born during a Zika virus outbreak on the islands from 2014 to 2015.
** Brazilian officials are also reporting neurological complications in other Zika virus patients, primarily Guillain-Barre syndrome.
** Guillain-Barre syndrome has also been seen in French Polynesian patients who had suspected Zika virus infections.
** There is no vaccine or treatment for Zika virus infection.

San Bernardino: A gunfight and the death of two suspects – a man and a woman
Thursday, December 3rd, 2015** The shooters were armed with long guns, wearing ski masks and military-style vests.
** A third suspect may still be at large;
Active Shooter Incident, San Bernardino: Up to 14 dead and 14 wounded; Multiple suspects fled scene.
Wednesday, December 2nd, 2015


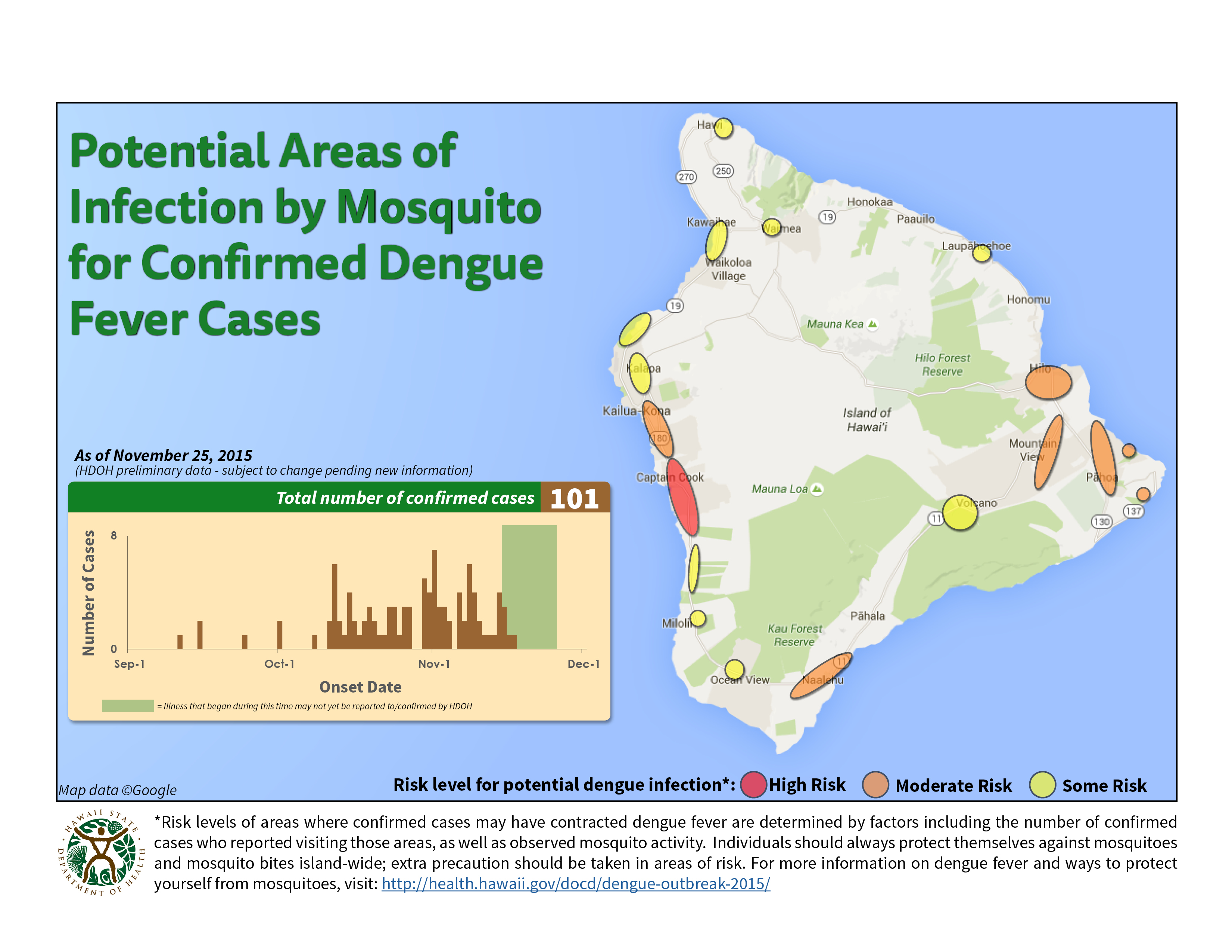
117 confirmed dengue cases in Hawaii
Wednesday, December 2nd, 2015The Hawaii Department of Health (HDOH) is investigating a cluster of locally-acquired cases of dengue fever on Hawaii Island. Dengue is not endemic to Hawaii. However, it is intermittently imported from endemic areas by infected travelers. This is the first cluster of locally-acquired dengue fever since the 2011 outbreak on Oahu.
As of December 1, 2015*:
| Hawaii Island residents | 103 |
| Visitors | 14 |
| Confirmed cases, TOTAL | 117 |
Of the confirmed cases, 103 are Hawaii Island residents and 14 are visitors.
88 cases have been adults; twenty-nine have been children (<18 years of age). Onset of illness has ranged between 9/11/15 – 11/20/15.