Archive for the ‘SFTS’ Category
Illnesses on the rise from mosquito, tick, and flea bites
Sunday, June 2nd, 2019Almost everyone has been bitten by a mosquito, tick, or flea. These can be vectors for spreading pathogens (germs). A person who gets bitten by a vector and gets sick has a vector-borne disease, like dengue, Zika, Lyme, or plague. Between 2004 and 2016, more than 640,000 cases of these diseases were reported, and 9 new germs spread by bites from infected mosquitoes and ticks were discovered or introduced in the US. State and local health departments and vector control organizations are the nation’s main defense against this increasing threat. Yet, 84% of local vector control organizations lack at least 1 of 5 core vector control competencies. Better control of mosquitoes and ticks is needed to protect people from these costly and deadly diseases.
State and local public health agencies can
- Build and sustain public health programs that test and track germs and the mosquitoes and ticks that spread them.
- Train vector control staff on 5 core competencies for conducting prevention and control activities. http://bit.ly/2FG1OMwExternal
- Educate the public about how to prevent bites and control germs spread by mosquitoes, ticks, and fleas in their communities.
Increasing threat, limited capacity to respond
More cases in the US (2004-2016)
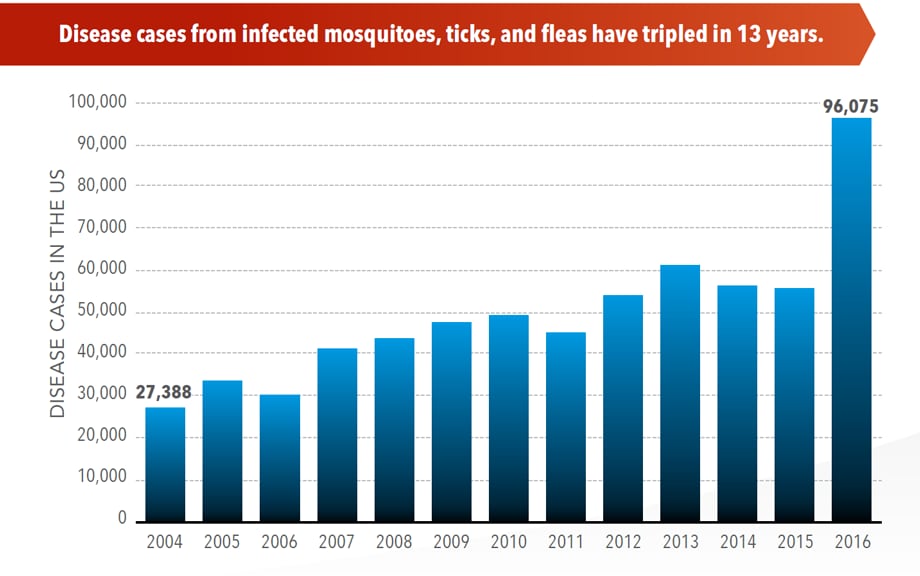
- The number of reported cases of disease from mosquito, tick, and flea bites has more than tripled.
- More than 640,000 cases of these diseases were reported from 2004 to 2016.
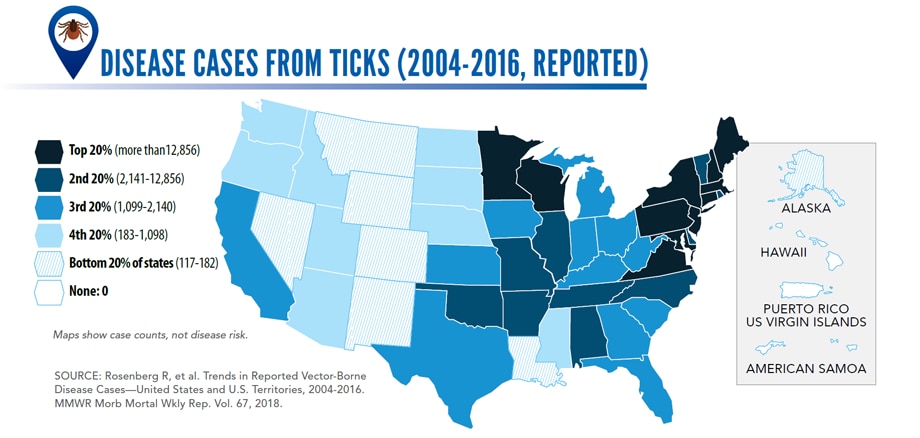
- Disease cases from ticks have doubled.
- Mosquito-borne disease epidemics happen more frequently.
More germs (2004-2016)
- Chikungunya and Zika viruses caused outbreaks in the US for the first time.
- Seven new tickborne germs can infect people in the US.
More people at risk
- Commerce moves mosquitoes, ticks, and fleas around the world.
- Infected travelers can introduce and spread germs across the world.
- Mosquitoes and ticks move germs into new areas of the US, causing more people to be at risk.
The US is not fully prepared
-
- Local and state health departments and vector control organizations face increasing demands to respond to these threats.
- More than 80% of vector control organizations report needing improvement in 1 or more of 5 core competencies, such as testing for pesticide resistance.
- More proven and publicly accepted mosquito and tick control methods are needed to prevent and control these diseases.
Severe Fever with Thrombocytopenia Syndrome in Vietnam
Saturday, April 27th, 2019Tran X, Yun Y, Van An L, Kim S, Thao NT, Man PC, et al. Endemic Severe Fever with Thrombocytopenia Syndrome, Vietnam. Emerg Infect Dis. 2019;25(5):1029-1031. https://dx.doi.org/10.3201/eid2505.181463
“…..Severe fever with thrombocytopenia syndrome virus (SFTSV) is a tickborne virus (genus Phlebovirus, family Phenuiviridae) that can cause a mild to severe febrile illness similar to hemorrhagic fever…..
On October 29, 2017, a 29-year-old woman (Hue 06-Vietnam-10-2017) was hospitalized at Hue University Hospital because of headache, vomiting, and gum bleeding. She lived in Hue City and was unaware of having received an insect bite. Her temperature was 38°C, and blood tests showed leukopenia (leukocyte count 1,900 cells/μL [reference 4,000–10,000 cells/μL]), thrombocytopenia (platelet count 125 × 103/μL [reference 150–450 × 103/μL]), and a low hematocrit level (34.3% [reference 36%–44%]). The patient fully recovered without other complications after 5 days.
On November 2, 2017, a 27-year-old man (Hue 13-Vietnam-11-2017) was hospitalized at Hue University Hospital because of headache and fatigue. He had had dengue fever at 8 years of age. Blood tests showed thrombocytopenia (platelet count 14 × 103/μL), normal leukocyte count (7,410 cells/μL), mildly elevated aspartate aminotransferase (84 IU/L [reference 8–38 IU/L]), elevated alanine aminotransferase (98 IU/L [reference 4–44 IU/L]), and mildly elevated hematocrit (47.6% [reference 36%–44%]). He fully recovered without other complications after 7 days…….”
Latest research indicates that SFTSV can be transmitted from person to person through aerosols.
Friday, January 18th, 2019Moon J, et al. (2018). Aerosol transmission of severe fever with thrombocytopenia syndrome virus during resuscitation. Infection Control & Hospital Epidemiology. 2018: 1–4. doi: 10.1017/ice.2018.330
“…..During aerosol generating procedures, SFTSV was be transmitted from person to person through aerosols. Thus, airborne precautions should be added to standard precautions to avoid direct contact and droplet transmission……”
Abstract
Severe fever with thrombocytopenia syndrome (SFTS) caused by SFTS virus (SFTSV), a novel phlebovirus, was reported to be endemic to central and northeastern PR China and was also to be endemic to South Korea and western Japan. SFTS is an emerging viral infection, which should be categorized as a viral hemorrhagic fever disease as Crimean-Congo hemorrhagic fever (CCHF) is caused by CCHF virus. SFTS is a tick-borne viral infection. SFTSV is maintained between several species of ticks and wild and domestic animals in nature. Patients with SFTS show symptoms of fever, general fatigue, and gastrointestinal symptoms such as bloody diarrhea. The severely ill SFTS patients usually show gastrointestinal hemorrhage and deteriorated consciousness. The case fatality rate of SFTS ranges from 5 to 40%. Pathological studies on SFTS have revealed that the mechanisms behind the high case fatality rate are virus infection-related hemophagocytic syndrome associated with cytokine storm, coagulopathy due to disseminated intravascular coagulation causing bleeding tendency, and multi-organ failure. Favipiravir was reported to show efficacy in the prevention and treatment of SFTSV infections in an animal model. A clinical study to evaluate the efficacy of favipiravir in the treatment of SFTS patients has been initiated in Japan. SFTSV is circulating in nature in PR China, Korea, and Japan, indicating that we cannot escape from the risk being infected with SFTSV. The development of specific therapy and preventive measures is a pressing issue requiring resolution to reduce the morbidity and mortality of SFTS patients.
A veterinarian and a veterinary nurse from the same Japanese animal clinic contracted severe fever with thrombocytopenia syndrome (SFTS) after treating a cat that was infected with the tickborne virus.
Friday, December 14th, 2018Abstract
Severe fever with thrombocytopenia syndrome (SFTS) is an emerging infectious disease caused by SFTS virus (SFTSV). SFTSV is associated with a high mortality rate and has been reported in China, South Korea and Japan. SFTSV undergoes rapid changes owing to evolution, gene mutations, and reassortment between different strains of SFTSV. In this review, we summarize the recent cases and general properties of SFTS, focusing on the epidemiology, genetic diversity, clinical features, and diagnostics of SFTSV in China. From 2010 to October 2016, SFTS cases were reported in 23 provinces of China, with increased numbers yearly. Infection and death cases are mainly found in central China, where the Haemaphysalis longicornis ticks are spread. The national average mortality rate of SFTS infection was 5.3%, with higher risk to elder people. The main epidemic period was from May to July, with a peak in May. Thus, SFTS reminds a significant public health problem, and development of prophylactic vaccines and effective antiviral drugs will be highly needed.
Exotic Disease–Vector Tick Haemaphysalis longicornis
Friday, November 30th, 2018Beard CB, Occi J, Bonilla DL, et al. Multistate Infestation with the Exotic Disease–Vector Tick Haemaphysalis longicornis — United States, August 2017–September 2018. MMWR Morb Mortal Wkly Rep 2018;67:1310–1313. DOI: http://dx.doi.org/10.15585/mmwr.mm6747a3.
“…..H. longicornis is native to eastern China, Japan, the Russian Far East, and Korea. It is an introduced, and now established, exotic species in Australia, New Zealand, and several island nations in the western Pacific Region. Where this tick exists, it is an important vector of human and animal disease agents. In China and Japan, it transmits the severe fever with thrombocytopenia syndrome virus (SFTSV), which causes a human hemorrhagic fever (2), and Rickettsia japonica, which causes Japanese spotted fever…..”
Counties and county equivalents* where Haemaphysalis longicornis has been reported (N = 45) — United States, August 2017–September 2018
| Host category, no. (% of total)/Species | No. (% of host category) |
|---|---|
| Domestic animal, 23 (61) | |
| Cat | 1 (4) |
| Cow | 4 (17) |
| Dog | 12 (52) |
| Goat | 2 (9) |
| Horse | 2 (9) |
| Sheep | 2 (9) |
| Total | 23 (100) |
| Wildlife, 13 (34) | |
| Coyote | 1 (8) |
| White-tailed deer | 7 (54) |
| Gray fox | 1 (8) |
| Groundhog | 1 (8) |
| Virginia opossum | 2 (15) |
| Raccoon | 1 (8) |
| Total | 13 (100) |
| Human, 2 (5) | 2 (100) |
| Total | 38 (100) |
WHO: Prioritizing Emerging Infectious Diseases in Need of Research and Development
Sunday, August 19th, 2018The World Health Organization R&D Blueprint aims to accelerate the availability of medical technologies during epidemics by focusing on a list of prioritized emerging diseases for which medical countermeasures are insufficient or nonexistent. The prioritization process has 3 components: a Delphi process to narrow down a list of potential priority diseases, a multicriteria decision analysis to rank the short list of diseases, and a final Delphi round to arrive at a final list of 10 diseases.
A group of international experts applied this process in January 2017, resulting in a list of 10 priority diseases. The robustness of the list was tested by performing a sensitivity analysis. The new process corrected major shortcomings in the pre–R&D Blueprint approach to disease prioritization and increased confidence in the results.
 Disease final ranking using the geometric average of the comparison matrices. B) Disease final ranking using the arithmetic average of the raw data. Error bars correspond to SD, indicating disagreement among experts. C) Disease final ranking using the SMART Vaccines prioritization tool (56). P1, Ebola virus infection; P2, Marburg virus infection; P3, Middle East Respiratory Syndrome coronavirus infection; P4, severe acute respiratory syndrome; P5, Lassa virus infection; P6, Nipah virus infection; P7, Rift Valley fever; P8, Zika virus infection; P9, Crimean-Congo hemorrhagic fever; P10, severe fever with thrombocytopenia syndrome; P11, South American hemorrhagic fever; P12, plague; P13, hantavirus infection.")
Multicriteria scores of diseases considered in the 2017 prioritization exercise for the development of the World Health Organization R&D Blueprint to prioritize emerging infectious diseases in need of research and development. A) Disease final ranking using the geometric average of the comparison matrices. B) Disease final ranking using the arithmetic average of the raw data. Error bars correspond to SD, indicating disagreement among experts. C) Disease final ranking using the SMART Vaccines prioritization tool (56). P1, Ebola virus infection; P2, Marburg virus infection; P3, Middle East Respiratory Syndrome coronavirus infection; P4, severe acute respiratory syndrome; P5, Lassa virus infection; P6, Nipah virus infection; P7, Rift Valley fever; P8, Zika virus infection; P9, Crimean-Congo hemorrhagic fever; P10, severe fever with thrombocytopenia syndrome; P11, South American hemorrhagic fever; P12, plague; P13, hantavirus infection.
Si Mehand M, Millett P, Al-Shorbaji F, Roth C, Kieny MP, Murgue B. World Health Organization methodology to prioritize emerging infectious diseases in need of research and development. Emerg Infect Dis. 2018 Sep [date cited]. https://doi.org/10.3201/eid2409.171427
An Invasive New Tick Comes to the USA
Thursday, August 9th, 2018“…..In East Asia, long-horned ticks do carry pathogens related to Lyme and others found in North America. But the biggest threat is a phlebovirus that causes S.F.T.S., for severe fever with thrombocytopenia syndrome…..The syndrome has an overall fatality rate of about 15 percent….But S.F.T.S. is more lethal to people aged 60 or older, killing half of them..…..”
 from case-patients, South Korea, 2013. A, B) Indirect immunofluorescent features of Vero E6 cells primed with SFTSV N protein monoclonal antibody and reacted with fluoresce in isothiocyanateconjugated anti-mouse IgG. B) Transmission electron microscopy image of Vero E6 cells infected with SFTSV. Scale bar indicates 500 nm.")
Severe fever with thrombocytopenia syndrome in China, 2011–17
Thursday, July 26th, 2018“…..Between April 1, 2011, and Oct 31, 2017, 2096 patients with laboratory-confirmed SFTS were admitted. Mean age at admission was 61·4 years (SD 12·2) and 1239 (59%) patients were female. The case fatality rate (CFR) was 16·2% (95% CI 14·6–17·8). A higher risk was associated with being male (unadjusted odds ratio [OR] 1·45, 95% CI 1·15–1·83; p=0·002), older age (for a 10-year increase, unadjusted OR 1·82, 95% CI 1·62–2·04; p<0·0001), longer delay in admission (for every extra day taken before admission to hospital, unadjusted OR 1·18, 1·12–1·24; p<0·0001), presence of diarrhoea (adjusted OR 1·44, 1·12–1·87; p=0·005) or dyspnoea (adjusted OR 8·35, 5·97–11·69; p<0·0001), and development of haemorrhagic signs (adjusted OR 2·79, 95% CI 2·18–3·57; p<0·0001) or neurological symptoms (adjusted OR 30·26, 21·39–42·81; p<0·0001). Laboratory variables that were associated with death included abnormal concentrations of lactate dehydrogenase, aspartate aminotransferase, and blood urea nitrogen, and abnormal neutrophil percentage, which together with age and neurological symptoms were combined in the clinical scoring system. A total score of more than 8 was the optimal threshold to predict risk of death for patients who were evaluated within 6 days after symptom onset (area under the curve 0·879, 95% CI 0·855–0·902). For all participants, viraemia was a strong predictor of fatal outcome (all p<0·0001). Ribavirin therapy was effective in reducing CFR from 6·25% (15 of 240 participants) to 1·16% (two of 173 participants), but only in patients with a viral load below 1×106 copies per mL (hazard ratio 9·72, 95% CI 1·30–72·87; p=0·027)……”

SFTS (severe fever with thrombocytopenia syndrome): A Japanese woman has died from a tick-borne virus after being bitten by a stray cat in what is possibly the world’s first animal-to-human transmission of the disease.
Saturday, July 29th, 2017- “….In Japan some 60 people contract the disease every year from tick bites with a fatality rate of some 20 percent….”
- Zhao L, Zhai S, Wen H, Cui F, Chi Y, Wang L, et al. Severe Fever with Thrombocytopenia Syndrome Virus, Shandong Province, China. Emerg Infect Dis. 2012;18(6):963-965. https://dx.doi.org/10.3201/eid1806.111345
-
Park S, Han M, Yun S, Park C, Lee W, Ryou J, et al. Severe Fever with Thrombocytopenia Syndrome Virus, South Korea, 2013. Emerg Infect Dis. 2014;20(11):1880-1882. https://dx.doi.org/10.3201/eid2011.140888
Isolation of severe fever with thrombocytopenia syndrome virus (SFTSV) from case-patients, South Korea, 2013. A, B) Indirect immunofluorescent features of Vero E6 cells primed with SFTSV N protein monoclonal antibody and reacted with fluoresce in isothiocyanateconjugated anti-mouse IgG. B) Transmission electron microscopy image of Vero E6 cells infected with SFTSV. Scale bar indicates 500 nm.