
Archive for April, 2016
Pakistan: A suicide bomber has attacked a government office in Mardan, wounding at least 10 people, 3 critically.
Tuesday, April 19th, 2016The first bombing on an Israeli bus in years appears to be an act of terrorism, according Israeli police.
Tuesday, April 19th, 2016A Taliban suicide car bomber kills at least 28 and injures more than 300 in Kabul, Afghanistan
Tuesday, April 19th, 2016“…..Even as the Taliban stretch Afghan forces throughout the country, with fighting raging across multiple provinces, complex urban attacks remain crucial to their insurgency. The pattern is often the same: After a vehicle-borne explosion creates chaos and an entry to their target building, militants equipped with weapons and suicide vests storm in and fight until the police, and the elite Crisis Response Unit, kill them and clear the area…..”

Ecuador’s 7.8M earthquake: The death toll soared to 238 on Sunday afternoon — and it’s expected to rise. At least 1,500 people are injured.
Sunday, April 17th, 2016


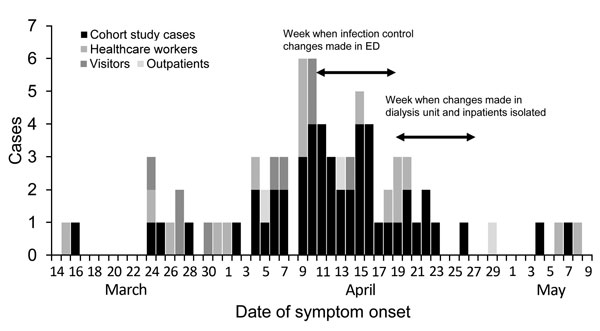
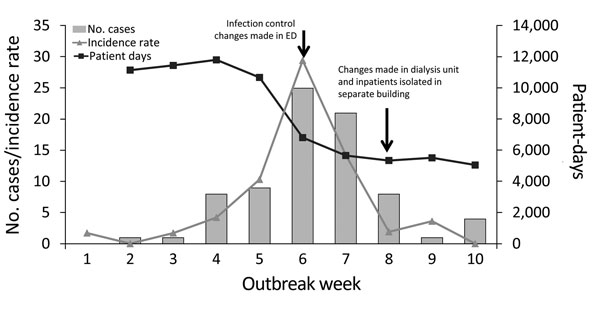
MMWR: Outbreak of Middle East Respiratory Syndrome at Tertiary Care Hospital, Jeddah, Saudi Arabia, 2014
Sunday, April 17th, 2016Hastings DL, Tokars JI, Abdel Aziz IZAM, Alkhaldi KZ, Bensadek AT, Alraddadi BM, et al. Outbreak of Middle East respiratory syndrome at tertiary care hospital, Jeddah, Saudi Arabia, 2014. Emerg Infect Dis. 2016 May [date cited]. http://dx.doi.org/10.3201/eid2205.151797
** “…78 people with confirmed MERS-CoV…linked to the hospital from Mar 2 to May 10, 2014. Most cases involved patients (68%, or 53), and the other infections occurred in healthcare workers (20.5%, or 16) and hospital visitors (11.5%, or 9). Many of the infected healthcare workers were physicians (63%, or 10)…”
** “….Infection control deficiencies included limited separation of suspected MERS patients, patient crowding, and inconsistent use of infection control precautions….”
** “…An aggressive program involving patient triage, use of negative-pressure isolation rooms, patient spacing in dialysis units, and personal protective equipment protocol in April 2014 led to a drastic decline in KFGH MERS cases….”
** YF in Angola: As of 7 April 2016, a total of 1,708 suspected cases, including 238 deaths (CFR: 13.9%).
Sunday, April 17th, 2016Yellow fever – Angola
On 21 January 2016, the National IHR Focal Point of Angola notified WHO of an outbreak of yellow fever (YF). The first case with onset date on 5 December 2015 was identified in Viana municipality, Luanda province.
As of 7 April 2016, a total of 1,708 suspected cases, including 238 deaths (CFR: 13.9%), had been reported from 16 of the country’s 18 provinces. Luanda remains the most affected province with 1,135 cases (405 confirmed), including 165 deaths (CFR: 14. 5%). The other most affected provinces are Huambo (266 suspected cases, 37 deaths), Huila (95 suspected cases, 16 deaths) and Benguela (51 suspected cases, 0 deaths). Between 6 and 7 April, 30 new suspected cases, including 4 deaths, were reported across the country – 19 of these suspected cases and 2 of the reported deaths came from Luanda.
A total of 581 cases have been laboratory confirmed in 59 districts of 12 provinces. Luanda province, the epicentre of the outbreak, accounts for 70% of the confirmed cases (405 cases). Other provinces with a high number of confirmed cases include Huambo (73 cases), Huila (27 cases), Benguela (22 cases) and Kuanza Sul (11 cases). From 6 to 7 April, 30 new confirmed cases were reported from Luanda (19), Huambo (4), Cuanza Sul (2), Cunene (2), Bengo (1), Lunda Norte (1) and Uige (1). The number of laboratory confirmed cases in provinces other than Luanda continues to increase. The risk of spread to other provinces and to neighbouring countries remains very high.
Transmission of the disease is no longer restricted to Luanda. As of 7 April 2016, the National Final Classification Committee had confirmed local transmission in five other provinces (Benguela, Cuanza Sul, Huambo, Huila and Uige) and in a total of 10 districts.
In addition, international spread of the disease has already been documented. Recent imported cases of YF have in fact been detected in China, Kenya and the Democratic Republic of the Congo (DRC) (see DONs published on 11 and 6 April).
Public health response
A national task force established by the government of Angola is leading the response to the outbreak. On 29 March, WHO graded the outbreak as a level 2 emergency on the Emergency Response Framework (ERF) grading scale – the ERF grading scale has three levels. WHO and partner organizations, including UNICEF, the Centers for Disease Control and Prevention, Médecins Sans Frontières (MSF) and Medicos del Mundo, are providing assistance with the coordination of the response. An incident manager has been appointed at WHO and 65 WHO multidisciplinary experts have been deployed to provide high-level technical support to the country.
Between 3 and 6 April, the WHO Director General, the WHO Regional Director for Africa and the WHO AFRO Health Security and Emergencies cluster Director visited Angola to assess the ongoing response and provide high-level leadership support. The delegation met the Minister of Health, other Government Officials and His Excellency the President of the Republic of Angola. Decisions were made to take necessary measures to end the outbreak by 15 May 2016.
Interventions are ongoing to enhance surveillance. These include epidemiological investigation, data management, early detection and confirmation of cases as well as final classification of cases by an established classification committee. Experts from Cuba are providing technical support to the country with the training of vector control specialists.
The immunization campaign in Luanda, which started on 2 February in Viana municipality, has been completed in 7 out of the province’s 12 districts and is still ongoing in the remaining five districts. As of 7 April, a total of 5,892,901 (90%) people had been vaccinated in Luanda. Preparation has started for the upcoming yellow fever vaccination campaign in 2 districts of Huambo and 3 of Benguela. On 7 April, the International Coordinating Group (ICG) for Vaccine Provision released 1.9 million vaccine doses. The social mobilization activities are being reinforced. Radio, TV and other media are being used to raise public awareness and encourage people to get vaccinated, with a special focus on vulnerable areas in all districts of Luanda.
The United Nations Central Emergency Response Fund (CERF) has approved a request of 3 million dollars to support the purchase of vaccines. In addition, the government of Angola has committed 15 million USD for the purchase of the yellow fever vaccine in addition to the payment of the 50% of the cost of the vaccines already received for the province of Luanda.
Current challenges include the need of vaccines to complete reactive immunization, the control of the geographical spread of the outbreak within the country and to neighbouring countries. There also needs for more operational funds, adequate and sufficient vector control interventions to improve response activities in the other provinces. A close follow-up of preparedness measures in neighbouring countries is required to ensure the timely detection and management of any imported cases.
WHO risk assessment
The evolution of the situation in Angola is concerning and needs to be closely monitored.
The reports of imported cases of YF in China, DRC and Kenya demonstrate that this outbreak constitutes a potential threat for the entire world.
There is a risk for the further spread of the disease in view of the large international communities residing in Angola and the frequent travel activities with neighbouring and overseas countries. Furthermore, all countries where the mosquito vector (Aedes species) is present are at risk, notably those endemic for or previously affected by outbreaks of Dengue, Chikungunya or Zika virus and other arboviruses. Therefore, there is an urgent need to strengthen the quality of the response in Angola and to enhance preparedness activities in neighbouring countries and in countries that have diaspora communities in Angola. WHO continues to monitor the epidemiological situation and conduct risk assessment based on the latest available information.
WHO advice
WHO urges Members States especially those where the establishment of a local cycle of transmission is possible (i.e., where the Aedes mosquitoes are present) to strengthen the control of immunization status of travellers to all potentially endemic areas and the surveillance of potential YF cases.
In the context of an ongoing YF outbreak in Angola, special attention should also be placed on travellers returning from Angola and other potentially endemic areas. Travellers, particularly those arriving in Asia from Africa or Latin America should always have a certificate of YF vaccination. If there are medical grounds for not getting vaccinated, the International Health Regulations (2005) state that this must be certified by the appropriate authorities.
WHO does not recommend any restriction of travel and trade to Angola based on the current information available.