Archive for March, 2017
CDC adds 4 nations to Zika travel guidance: Angola, Guinea-Bissau, Maldives, and Solomon Island
Sunday, March 12th, 2017
Mar 10 CDC travel advisory for Angola

Mar 10 CDC travel advisory for Guinea-Bissau

Mar 10 CDC travel advisory for Maldives

Mar 10 CDC travel advisory for Solomon Islands
China: 22 additional human cases of H7N9, including three deaths, were recorded from March 3 to 9.
Sunday, March 12th, 2017
WHO: 3 African nations—Benin, Togo, and Burkina Faso—have reported recent cases of Lassa fever that could foretell more outbreaks in the region.
Sunday, March 12th, 2017Lassa Fever – Benin, Togo and Burkina Faso
Benin and Togo, exported from Benin
On 20 February 2017, the Ministry of Health of Benin notified WHO of a Lassa fever case in Tchaourou district, Borgou Department, Benin, close to the border with Nigeria. The case was a pregnant woman who was living in Nigeria (close to the border with Benin).
On 11 February 2017, she was admitted to a hospital where she delivered the baby (a premature neonate) by caesarean section and passed away on 12 February 2017. Samples were tested positive for Lassa fever in the laboratory in Cotonou, Benin and later in the Lagos University Teaching Hospital Lassa laboratory in Nigeria. The newborn and father left the hospital without notice on 14 February 2017 and went to Mango in northern Togo where they were admitted to a hospital.
The newborn tested positive for Lassa fever and the father tested negative in the Institut National d’Hygiène in Lomé, Togo. The baby was treated with ribavirin and is currently in stable condition; he is still hospitalised in northern Togo for issues of prematurity and overall monitoring.
A total of 68 contacts are being followed-up in Benin and 29 contacts are being followed-up in Togo linked to the pregnant woman and newborn.
Togo, exported from Burkina Faso
On 26 February 2017, after receiving information from Togo, the Ministry of Health of Burkina Faso has notified WHO of a confirmed Lassa fever case in a hospital in the northern part of Togo. The case has originated from Ouargaye district which is in the central eastern part of Burkina Faso.
The case was a pregnant woman who was previously hospitalized in Burkina Faso. She was discharged and had a miscarriage at home. After the second hospitalization in Burkina Faso she was transmitted to a hospital in Mango, northern Togo, and passed away on 3 March 2017.
Samples from the pregnant woman tested positive for Lassa fever at the Institut National d’Hygiène in Lomé, Togo.
A total of 7 contacts have been identified in Togo linked to the pregnant woman and contact tracing is ongoing; 135 contacts in Burkina Faso have been identified linked to the pregnant woman and contact tracing is ongoing.
Togo
On 2 March 2017, a man was admitted to a health centre in the Kpendial health district for fever and melena and was referred to a regional hospital on 3 March 2017.
Samples from the male case were sent to the Institut National d’Hygiène in Lomé, Togo, and tested positive for Lassa fever. The case left the hospital on 6 March. Investigations are ongoing. The male case and his close relatives are under follow up at their home.
A total of 18 contacts were identified in Togo linked to the male case.
Public health response
Health authorities in Benin, Burkina Faso and Togo are implementing the following measures to respond to these Lassa fever cases, including:
- Deployment of rapid response teams to the affected areas for epidemiological investigation.
- Identification of contacts and follow-up.
- Strengthening of infection prevention and control measures in health facilities and briefing of health workers.
- Strengthening of cross border collaboration and information exchanges between Togo, Burkina, Mali and Benin.
WHO risk assessment
Lassa fever is an acute viral haemorrhagic fever illness. The Lassa virus is transmitted to humans via contact with food or household items contaminated with rodent urine or faeces. Person-to-person infections and laboratory transmission can also occur.
Lassa fever is endemic in neighbouring Nigeria and other West African countries and causes outbreaks almost every year in different parts of the region, with yearly peaks observed between December and February. The most recent Lassa fever outbreak in Benin occurred in the same area in January – May 2016. At least 54 cases including 28 deaths have been reported at country level. Both Burkina Faso and Togo have reported sporadic cases in the past.
Given constant important population movements between Nigeria, Togo, Burkina Faso, Niger and Benin, the occurrence of sporadic Lassa fever cases in West Africa was expected and further sporadic cases may occur in countries of the region.
However, with the ongoing control measures in Benin, Togo and Burkina Faso the risk of further disease spread from these confirmed cases is considered to be low. Considering the seasonal peaks in previous years, increase in the disease awareness, better preparedness and response in general, and strengthening of regional collaboration the risk of large scale outbreaks in the region is medium.
WHO advice
Prevention of Lassa fever relies on promoting good “community hygiene” to discourage rodents from entering homes. In health-care settings, staff should always apply standard infection prevention and control precautions when caring for patients, regardless of their presumed diagnosis.
On rare occasions, travellers from areas where Lassa fever is endemic export the disease to other countries. Although other tropical infections are much more common, the diagnosis of Lassa fever should be considered in febrile patients returning from West Africa, especially if they have had exposures in rural areas or hospitals in countries where Lassa fever is known to be endemic. Health-care workers seeing a patient suspected to have Lassa fever should immediately contact local and national experts for advice and to arrange for laboratory testing.
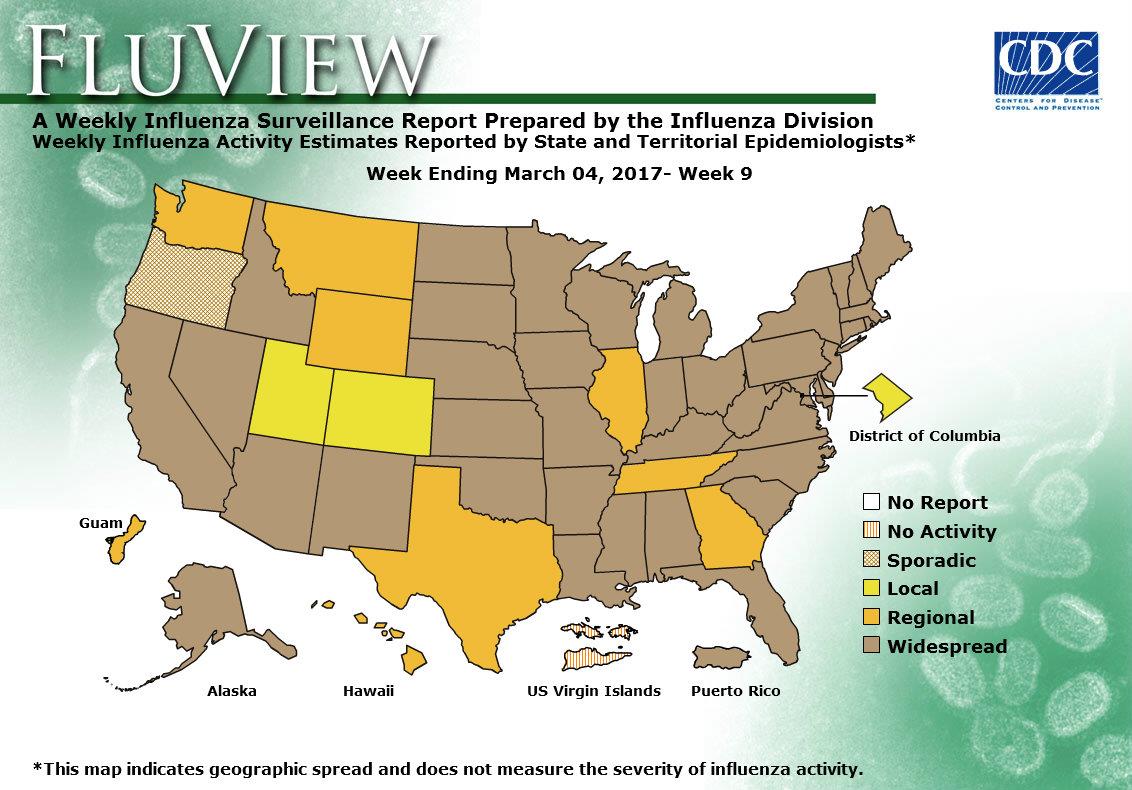
CDC: During week 9 (February 26-March 4, 2017), influenza activity decreased, but remained elevated in the United States.
Saturday, March 11th, 2017Synopsis:
During week 9 (February 26-March 4, 2017), influenza activity decreased, but remained elevated in the United States.
- Viral Surveillance: The most frequently identified influenza virus subtype reported by public health laboratories during week 9 was influenza A (H3). The percentage of respiratory specimens testing positive for influenza in clinical laboratories decreased.
- Pneumonia and Influenza Mortality: The proportion of deaths attributed to pneumonia and influenza (P&I) was above the system-specific epidemic threshold in the National Center for Health Statistics (NCHS) Mortality Surveillance System.
- Influenza-associated Pediatric Deaths: Eight influenza-associated pediatric deaths were reported.
- Influenza-associated Hospitalizations: A cumulative rate for the season of 43.5 laboratory-confirmed influenza-associated hospitalizations per 100,000 population was reported.
- Outpatient Illness Surveillance: The proportion of outpatient visits for influenza-like illness (ILI) was 3.6%, which is above the national baseline of 2.2%. Eight of ten regions reported ILI at or above their region-specific baseline levels. 14 states experienced high ILI activity; 12 states experienced moderate ILI activity; eight states experienced low ILI activity; New York City, Puerto Rico, and 16 states experienced minimal ILI activity; and the District of Columbia had insufficient data.
- Geographic Spread of Influenza: The geographic spread of influenza in Puerto Rico and 39 states was reported as widespread; Guam and eight states reported regional activity; the District of Columbia and two states reported local activity; one state reported sporadic activity; and the U.S. Virgin Islands reported no activity.
WHO: Zika virus, Microcephaly and Guillain-Barré syndrome
Saturday, March 11th, 2017Key updates
- Countries, territories and subnational areas reporting vector-borne Zika virus (ZIKV) infections for the first time since 1 February:
- None
- Countries and territories reporting microcephaly and other central nervous system malformations potentially associated with ZIKV infection for the first time since 1 February:
- Mexico, Saint Martin
- Countries and territories reporting Guillain-Barré syndrome cases associated with ZIKV infection for the first time since 1 February:
- Curaçao, Trinidad and Tobago
- WHO, the United States Centers for Disease Control and Prevention and the European Centre for Disease Prevention and Control have developed a new Zika virus classification scheme. The classification serves to categorize the presence of and potential for vector-borne ZIKV transmission and to inform public health recommendations. Based on the defined criteria and expert review, some countries, territories and subnational areas were reclassified and some were classified for the first time.
- In line with WHO’s transition to a sustained programme to address the long-term nature of the disease and its consequences, this is the final WHO Zika situation report. WHO will continue to publish the Zika classification table (Table 1) on a regular basis as well as periodic situation analysis.
World Tourism Network on Child Protection
Saturday, March 11th, 2017World Tourism Network on Child Protection
The World ![]() Tourism Network on Child Protection (formerly the Task Force for the Protection of Children in Tourism) is an open-ended network featuring the multi-stakeholder participation of a range of tourism stakeholders, from governments, international organisations and non-governmental organisations (NGOs) to tourism industry groups and media associations. Originally formed in 1997, since 2007 its mandate has been to prevent all forms of youth exploitation in the tourism sector (i.e. sexual exploitation, child labour and child trafficking). ….
Tourism Network on Child Protection (formerly the Task Force for the Protection of Children in Tourism) is an open-ended network featuring the multi-stakeholder participation of a range of tourism stakeholders, from governments, international organisations and non-governmental organisations (NGOs) to tourism industry groups and media associations. Originally formed in 1997, since 2007 its mandate has been to prevent all forms of youth exploitation in the tourism sector (i.e. sexual exploitation, child labour and child trafficking). ….
The activities of the World Tourism Network on Child Protection are co-ordinated by the UNWTO Secretariat and monitored by an Executive Committee established in November 2000.
Mission Statement and Objectives
Under the guiding principles of the Global Code of Ethics for Tourism, the mission of the World Tourism Network on Child Protection is to support efforts to protect children from all forms of exploitation in tourism. Although its main focus is the protection of minors against sexual exploitation, it encompasses the issues of child labour and the trafficking of minors. Its principle objectives are:
- to raise awareness among the tourism sector, governments and tourists;
- to encourage the tourism industry to engage in ethical practices, particularly by adopting professional codes of conduct and other self-regulatory measures;
- to invite governments to take administrative and legal measures, such as the designation of focal points (contact persons) within their national tourism administrations, the establishment of emergency hotlines, the strengthening of national legislation and the improvement of law enforcement;
- to encourage cooperation between the public and private sectors, as well as between tourist generating and receiving countries; and
- to monitor the fight against the sexual exploitation of children in tourism networks at both the national and international levels.
History of the World Tourism Network on Child Protection
The World Tourism Network on Child Protection was established as a “Task Force” by the World Tourism Organization in March 1997 at the ITB Berlin Tourism Fair in Germany, as a follow-up to the Stockholm Congress against the Commercial Sexual Exploitation of Children (1996). Two months later, the Task Force launched the international campaign “NO Child Sex Tourism” to combat the commercial sexual abuse of children in tourism by raising awareness of this unacceptable phenomenon. The logo for this campaign was provided by the Brazilian Tourist Board EMBRATUR. First presented to the media in Chantilly, France, during the “Salon mondial du tourisme” fair.
During its first phase (1997-2007), the focus of the body was the prevention of sexual exploitation of children in tourism. In March 2007, at the 20th Task Force meeting held in Berlin, Germany, its mandate was extended to cover all forms of exploitation of minors in tourism, including child labour and child trafficking. The name of the Task Force was changed to “World Tourism Network on Child Protection” in 2011.
- October 1995 – Member States of the World Tourism Organization take a stand against the sexual exploitation of children in tourism by unanimously adopting the Statement on the Prevention of Organized Sex Tourism at the General Assembly in Cairo, Egypt.
- August 1996 – The Stockholm Congress against Commercial Sexual Exploitation of Children introduces its Agenda for Action, which urged all participants to:
- mobilize the business sector, including the tourism industry, against the use of its networks and establishments for the commercial sexual exploitation of children; and
- promote better co-operation and encourage the establishment of national and international coalition to this effect.
- At the Congress, as many as 122 countries agreed to undertake measures to curb the commercial sexual exploitation of children. Several tourism industry associations (IATA; IFTO, IH&RA, UFTAA, etc.), also issued policy documents explicitly addressing this topic.
Yemen: UNICEF vaccination campaign reaches five million children
Saturday, March 11th, 2017“….In the first campaign of its kind this year, 40,000 vaccinators spread across Yemen to provide children with polio vaccine and vitamin A supplements. Mobile health teams have reached children wherever they are, including in places where access to health services has been cut off by the fighting. Health workers have shown heroic resolve in crossing frontlines, mountains and valleys to vaccinate children…..”
 Photo: UNICEF/UN026952/Madhok")
A little boy is vaccinated against polio in Sa’ada, Yemen. (file) Photo: UNICEF/UN026952/Madhok
“Starving to death”: UN aid chief urges global action as starvation, famine loom for 20 million across Kenya, Yemen, South Sudan and Somalia
Saturday, March 11th, 2017
10 March 2017 – Just back from Kenya, Yemen, South Sudan and Somalia – countries that are facing or are at risk of famine – the top United Nations humanitarian official today urged the international community for comprehensive action to save people from simply “starving to death.”
“We stand at a critical point in history. Already at the beginning of the year we are facing the largest humanitarian crisis since the creation of the UN,” UN Emergency Relief Coordinator Stephen O’Brien told the Security Council today.
Without collective and coordinated global efforts, he warned, people risk starving to death and succumbing to disease, stunted children and lost futures, and mass displacements and reversed development gains.
“The appeal for action by the Secretary-General can thus not be understated. It was right to sound the alarm early, not wait for the pictures of emaciated dying children […] to mobilize a reaction and the funds,” Mr. O’Brien underscored, calling for accelerated global efforts to support UN humanitarian action on the ground.
Turning to the countries he visited, the senior UN official said that, about two-thirds of the population (more than 18 million people) in Yemen needed assistance, including more than seven million severely food insecure, and the fighting continued to worsen the crisis.
“I continue to reiterate the same message to all: only a political solution will ultimately end human suffering and bring stability to the region,” he said, noting that with access and funding, humanitarians will do more, but cautioned that relief-workers were “not the long-term solution to the growing crisis.”
In South Sudan, where a famine was recently declared, more than 7.5 million people are in need of assistance, including some 3.4 million displaced. The figure rose by 1.4 million since last year.
“The famine in the country is man-made. Parties to the conflict are parties to the famine – as are those not intervening to make the violence stop,” stressed Mr. O’Brien, calling on the South Sudanese authorities to translate their assurances of unconditional access into “action on the ground.”
Similarly, more than half the population of Somalia (6.2 million people) is need aid, 2.9 million of whom require immediate assistance. Extremely worrying is that more than one million children under the age of five are at the risk of acute malnourishment.
“The current indicators mirror the tragic picture of 2011, when Somalia last suffered a famine,” recalled the UN official, but expressed hope that a famine can be averted with strong national leadership and immediate and concerted support by the international community.
Concerning Kenya, he mentioned that more than 2.7 million people were food insecure, and that this number could reach four million by April.
“In collaboration with the Government [of Kenya], the UN will soon launch an appeal of $200 million to provide timely life-saving assistance and protection,” he informed.
Further in his briefing, Mr. O’Brien informed the Council of the outcomes of the Oslo Conference on the Lake Chad Basin where 14 donors pledged a total of $672 million, of which $458 million is for humanitarian action in 2017.
“This is very good news, and I commend those who made such generous pledges,” he said but noted that more was needed to fully fund the $1.5 billion required to provide the assistance needed across the region.
On the UN response in these locations, Mr. O’Brien highlighted that strategic, coordinated and prioritized plans are in place and dedicated teams on the ground are closely working with partners to ensure that immediate life-saving support reaches those in need.
“Now we need the international community and this Council to act,” he highlighted, urging prompt action to tackle the factors causing famine; committing sufficient and timely financial support; and ensuring that fighting stops.
In particular, he underscored the need to ensure that humanitarians have safe, full and unimpeded access and that parties to the conflict in the affected countries respect humanitarian law and called on those with influence over the parties to the conflict to “exert that influence now.”
“It is possible to avert this crisis, to avert these famines, to avert these looming human catastrophes,” he concluded. “It is all preventable.”
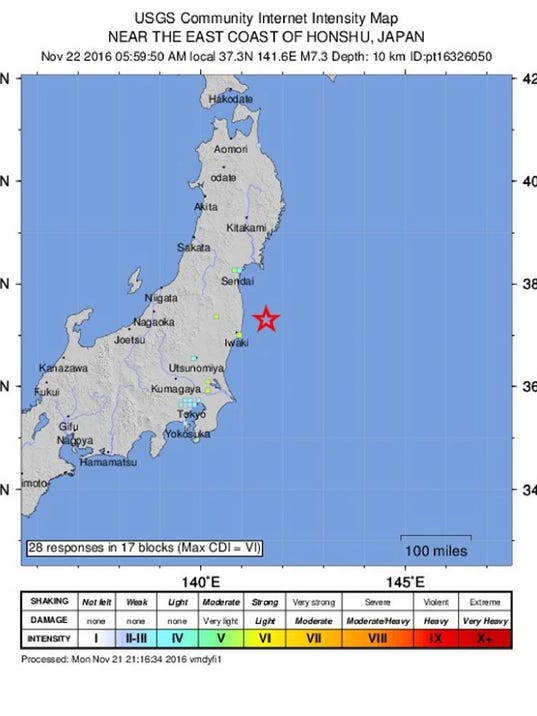
Signs of life are returning nearly six years after panicked residents fled radiation spewed by the nearby Fukushima Daiichi nuclear power plant, when it was struck by an earthquake and tsunami.
Friday, March 10th, 2017“….only several hundred of the original 21,500 residents plan to return in the first wave…”