Archive for April, 2017
Saudi Arabia: An outbreak of MERS occurred in a hemodialysis unit in a hospital in Riyadh. Contact tracing revealed that 8 symptomatic and 2 asymptomatic cases are associated with this outbreak.
Wednesday, April 5th, 2017Middle East respiratory syndrome coronavirus (MERS-CoV) – Saudi Arabia
Between 23 February and 16 March 2017 the national IHR focal point of Saudi Arabia reported 18 additional cases of Middle East Respiratory Syndrome (MERS) including two fatal cases. Four deaths among previously reported MERS cases were also reported (case numbers 1, 4, 5 and 7 in the Disease Outbreak News published on 10 March 2017).
An outbreak of MERS occurred in a haemodialysis unit in a hospital in Riyadh. Contact tracing revealed that eight symptomatic and two asymptomatic cases are associated with this outbreak.
Detailed information concerning the cases reported between 23 February and 16 March 2017 can be found in a separate document (see link below).
Globally, since September 2012, 1935 laboratory-confirmed cases of infection with MERS-CoV including at least 690 related deaths have been reported to WHO.
Public health response
In response to this outbreak, the rapid response team was dispatched from the Ministry of Health, and regional health directorate and this was followed by the activation of the outbreak management team.
The following measures were implemented:
- Intensive infection control training was given to all the hospital staff including the strict monitoring of infection control measures in the dialysis unit.
- Active triage of all haemodialysis patients prior to initiation of dialysis was enforced. Those with symptoms were directed to designated areas and managed as suspected cases.
- The haemodialysis unit was cleaned using hospital grade disinfectants and hydrogen peroxide fumigation.
- Asymptomatic patients served by the unit (or their caregivers) were contacted daily by phone to ensure they do not attend another haemodialysis unit or seek healthcare services elsewhere without coordination.
WHO risk assessment
MERS-CoV causes severe human infections resulting in high mortality and has demonstrated the ability to transmit between humans. So far, the observed human-to-human transmission has occurred mainly in health care settings.
The notification of additional cases does not change the overall risk assessment. WHO expects that additional cases of MERS-CoV infection will be reported from the Middle East, and that cases will continue to be exported to other countries by individuals who might acquire the infection after exposure to animals or animal products (for example, following contact with dromedaries) or human source (for example, in a health care setting). WHO continues to monitor the epidemiological situation and conducts risk assessment based on the latest available information.
WHO advice
Based on the current situation and available information, WHO encourages all Member States to continue their surveillance for acute respiratory infections and to carefully review any unusual patterns.
Infection prevention and control measures are critical to prevent the possible spread of MERS-CoV in health care facilities. It is not always possible to identify patients with MERS-CoV early because like other respiratory infections, the early symptoms of MERS-CoV are non-specific. Therefore, health-care workers should always apply standard precautions consistently with all patients, regardless of their diagnosis. Droplet precautions should be added to the standard precautions when providing care to patients with symptoms of acute respiratory infection; contact precautions and eye protection should be added when caring for probable or confirmed cases of MERS-CoV infection; airborne precautions should be applied when performing aerosol generating procedures.
Until more is understood about MERS-CoV, people with diabetes, renal failure, chronic lung disease, and immunocompromised persons are considered to be at high risk of severe disease from MERS-CoV infection. Therefore, these people should avoid close contact with animals, particularly camels, when visiting farms, markets, or barn areas where the virus is known to be potentially circulating. General hygiene measures, such as regular hand washing before and after touching animals and avoiding contact with sick animals, should be adhered to.
Food hygiene practices should be observed. People should avoid drinking raw camel milk or camel urine, or eating meat that has not been properly cooked.
WHO does not advise special screening at points of entry with regard to this event nor does it currently recommend the application of any travel or trade restrictions.
Syria: Witnesses to the attack said it began just after sunrise. Numerous photographs and graphic videos posted online by activists and residents showed children and older adults gasping and struggling to breathe, or lying motionless in the mud as rescue workers ripped off victims’ clothes and hosed them down. The bodies of least 10 children lay lined up on the ground or under a quilt.
Tuesday, April 4th, 2017“…..Rescue workers from the White Helmets civil defense organization said that many children were among at least 50 dead and 250 wounded. Radi Saad, who writes incident reports for the group, said that volunteers had reached the site not knowing a chemical was present, and that five of them had suffered from exposure to the substance…..”
St. Petersburg: The toll from the attack rose to 14 dead and more than 60 injured.
Tuesday, April 4th, 2017A different chemical attack in Syria? This time, people collapsed outdoors, and in much larger numbers. The symptoms were also different: They included the pinpoint pupils of victims that characterize nerve agents and other banned toxins. One doctor posted a video of a patient’s eye, showing the pupil reduced to a dot. Several people were sickened simply by coming into contact with the victims.
Tuesday, April 4th, 2017“….Numerous photographs and graphic videos posted online by activists and residents showed children and older adults gasping and struggling to breathe, or lying motionless in the mud as rescue workers ripped off victims’ clothes and hosed them down. The bodies of least 10 children lay lined up on the ground or under a quilt.
Rescue workers from the White Helmets civil defense organization said that many children were among at least 50 dead and 250 wounded…..”
CDC: Radiation Hazard Scale
Tuesday, April 4th, 2017…
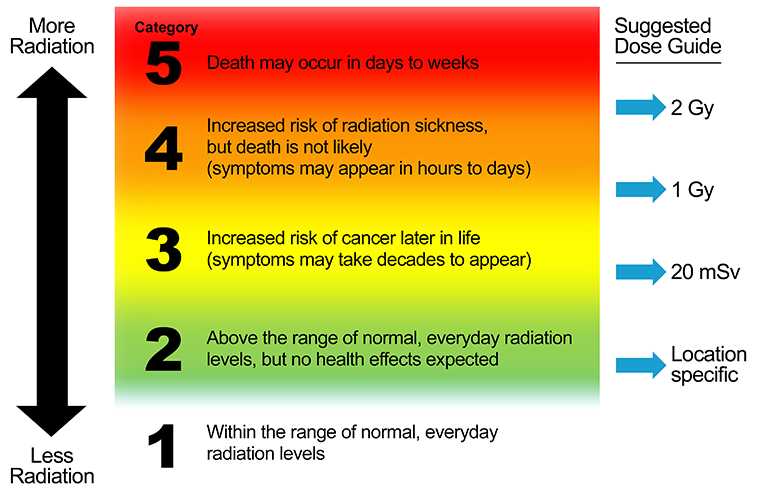
Radiation Hazard Scale
A Tool for Communication in Nuclear and Radiological Emergencies
The Centers for Disease Control and Prevention has developed the Radiation Hazard Scale as a tool for communication in emergencies.
This tool:
- Provides a frame of reference for relative hazards of radiation.
- Conveys meaning without using radiation measurements or units that are unfamiliar to people.
- Is designed for use only in radiation emergencies and is applicable for short-term exposure durations, for example, over a period of several days.
- Is best used when accompanied with protective action recommendations or instructions.
- Has been audience tested with public information officers, emergency management and public health professionals, and members of the public.

Description of the Radiation Hazard Scale Categories
Category |
Description |
| 5 |
Category 5 means that radiation doses are dangerously high and potentially lethal. High doses of radiation can cause massive damage to organs of the body and kill the person. The exposed person loses white blood cells and the ability to fight infections. Diarrhea and vomiting are likely. Medical treatment can help, but the condition may still be fatal in spite of treatment. At extremely high doses of radiation, the person may lose consciousness and die within hours. For more information, see https://www.remm.nlm.gov/ars_summary.htm |
| 4 |
Category 4 means that radiation doses are dangerously high and can make people seriously ill. Radiation doses are not high enough to cause death, but one or more symptoms of radiation sickness may appear. Radiation sickness, also known as Acute Radiation Syndrome (ARS), is caused by a high dose of radiation. The severity of illness depends on the amount (or dose) of radiation. The earliest symptoms may include nausea, fatigue, vomiting, and diarrhea. Symptoms such as hair loss or skin burns may appear in weeks. For more information about the health effects of radiation, see http://emergency.cdc.gov/radiation/healtheffects.asp For more information about medical treatment of radiation exposure, see http://emergency.cdc.gov/radiation/countermeasures.asp |
| 3 |
Category 3 means that radiation doses are becoming high enough where we may expect increased risk of cancer in the years ahead for people who are exposed. Leukemia and thyroid cancers can appear in as few as 5 years after exposure. Other types of cancer can take decades to develop. Studies have shown that radiation exposure can increase the risk of people developing cancer. This increased risk of cancer is typically a fraction of one percent. The lifetime risk of cancer for the population due to natural causes is approximately 40%. The increase in risk of cancer from radiation depends on the amount (or dose) of radiation, and it becomes vanishingly small and near zero at low doses of radiation. For more information, see http://emergency.cdc.gov/radiation/cancer.asp |
| 2 |
Category 2 means that radiation levels in the environment are higher than the natural background radiation for that geographic area. However, these radiation levels are still too low to observe any health effects. When radiation levels are higher than what we normally have in our natural environment, it does not necessarily mean that it will cause us harm. For more information about health effects of radiation, see http://www.cdc.gov/nceh/radiation/health.html |
| 1 |
Category 1 means that radiation levels in the environment are within the range of natural background radiation for that geographic area. Low amounts of radioactive materials exist naturally in our environment, food, air, water, and consequently in our bodies. We are also exposed to radiation from space that reaches the surface of the Earth. These conditions are natural, and this radiation is called the natural background radiation. For more information about radiation and radioactivity in everyday life and how it can vary by location, see http://www.cdc.gov/nceh/radiation/sources.html |
Suggested Guide on How to Assign Radiation Hazard Categories
The Radiation Hazard Scale is intended to communicate relative hazards to populations under emergency conditions when exact radiation exposure parameters for specific individuals are not available. Note that:
- There are no sharp lines separating radiation hazard categories.
- Transition from Category 1 to Category 2 depends on the range of natural background radiation for a geographic area.
- The radiation dose values are whole-body doses and are suggested guides for radiation protection purposes. Dose values are meant to be used by radiation protection experts and emergency response or public health authorities. For a description of radiation units listed in the dose guide, see Primer on Radiation Measurements.
- Radiation dose values are not meant to be included in public messaging, especially during early phase of a radiation emergency.
This guide is applicable for short-term exposure durations, for example, over a period of several days during an emergency.
Example Uses of Radiation Hazard Scale in Emergency Communication Messages
Examples after a nuclear detonation:
- In areas where the Radiation Hazard Category is 5, sheltering in place can help maintain a Category 2 or 3 until instructed to evacuate. In contrast, self-directed evacuation in fallout areas can place a person at Category 4 or 5.
- If people are contaminated with nuclear fallout, self-decontamination can rapidly decrease radiation hazard from Category 5 to Category 2 or 1.
Example Uses of Radiation Hazard Scale in Displaying Environmental Data
Select a scenario:
- Detonation of an Improvised Nuclear Device (IND) – Download PDF
- Accidental release from a nuclear power plant (NPP) – Download PDF
- Explosion of a Radiological Dispersal Device (RDD) – Download PDF
Frequently Asked Questions
What is the difference between the International Nuclear Event Scale (INES) and the Radiation Hazard Scale?
These two scales have quite different applications in an emergency. The INES, developed by the International Atomic Energy Agency is a tool to grade the safety significance of a particular event associated with sources of ionizing radiation. The INES describes the accident itself. On the other hand, the Radiation Hazard Scale describes the immediate potential impact of the accident for people, and the hazard category depends on where people are located.
For example, the severity of the March 2011 accident at the Fukushima Daiichi nuclear power plant has been given the highest rating of 7 on the INES scale. Regardless of whether we live in the United States or Japan, the INES rating for the Fukushima Daiichi accident is 7. However, the Radiation Hazard Category would have been quite different for people depending on their location. For emergency responders working at the Fukushima Daiichi plant at the time of the accident, the Radiation Hazard Category was 4 or 5 depending on where they worked at the plant. At the same time, the Radiation Hazard Category for people living in Tokyo was 2 for a short period of time, and it was Category 1 for people in the United States.
Can the radiation hazard scale be used to describe medical exposures?
No. In its present form, this Scale is intended only for emergency exposure situations.
Would the public need pre-event education on interpreting the scale?
While pre-event education is always helpful, there is no requirement for pre-event public education for effective use of this Scale. Our audience testing with members of the public who had at least a high school diploma indicated that the Scale is simple enough to understand, and it can be described briefly by a Public Information Officer or a news reporter.
Who would assign the radiation hazard categories in an emergency?
Environmental scientists and radiation safety experts can evaluate the data and assign the Radiation Hazard Categories in coordination with emergency management authorities, public health officials, and communication experts.
Lassa fever: WHO Review
Tuesday, April 4th, 2017Lassa fever
Key facts
- Lassa fever is an acute viral haemorrhagic illness of 2-21 days duration that occurs in West Africa.
- The Lassa virus is transmitted to humans via contact with food or household items contaminated with rodent urine or faeces.
- Person-to-person infections and laboratory transmission can also occur, particularly in hospitals lacking adequate infection prevent and control measures.
- Lassa fever is known to be endemic in Benin, Ghana, Guinea, Liberia, Mali, Sierra Leone, and Nigeria, but probably exists in other West African countries as well.
- The overall case-fatality rate is 1%. Observed case-fatality rate among patients hospitalized with severe cases of Lassa fever is 15%.
- Early supportive care with rehydration and symptomatic treatment improves survival.
Background
Though first described in the 1950s, the virus causing Lassa disease was not identified until 1969. The virus is a single-stranded RNA virus belonging to the virus family Arenaviridae.
About 80% of people who become infected with Lassa virus have no symptoms. 1 in 5 infections result in severe disease, where the virus affects several organs such as the liver, spleen and kidneys.
Lassa fever is a zoonotic disease, meaning that humans become infected from contact with infected animals. The animal reservoir, or host, of Lassa virus is a rodent of the genus Mastomys, commonly known as the “multimammate rat.” Mastomys rats infected with Lassa virus do not become ill, but they can shed the virus in their urine and faeces.
Because the clinical course of the disease is so variable, detection of the disease in affected patients has been difficult. When presence of the disease is confirmed in a community, however, prompt isolation of affected patients, good infection prevention and control practices, and rigorous contact tracing can stop outbreaks.
Lassa fever is known to be endemic in Benin (where it was diagnosed for the first time in November 2014), Ghana (diagnosed for the first time in October 2011), Guinea, Liberia, Mali (diagnosed for the first time in February 2009), Sierra Leone, and Nigeria, but probably exists in other West African countries as well.
Symptoms of Lassa fever
The incubation period of Lassa fever ranges from 6–21 days. The onset of the disease, when it is symptomatic, is usually gradual, starting with fever, general weakness, and malaise. After a few days, headache, sore throat, muscle pain, chest pain, nausea, vomiting, diarrhoea, cough, and abdominal pain may follow. In severe cases facial swelling, fluid in the lung cavity, bleeding from the mouth, nose, vagina or gastrointestinal tract and low blood pressure may develop.
Protein may be noted in the urine. Shock, seizures, tremor, disorientation, and coma may be seen in the later stages. Deafness occurs in 25% of patients who survive the disease. In half of these cases, hearing returns partially after 1–3 months. Transient hair loss and gait disturbance may occur during recovery.
Death usually occurs within 14 days of onset in fatal cases. The disease is especially severe late in pregnancy, with maternal death and/or fetal loss occurring in more than 80% of cases during the third trimester.
Transmission
Humans usually become infected with Lassa virus from exposure to urine or faeces of infected Mastomys rats. Lassa virus may also be spread between humans through direct contact with the blood, urine, faeces, or other bodily secretions of a person infected with Lassa fever. There is no epidemiological evidence supporting airborne spread between humans. Person-to-person transmission occurs in both community and health-care settings, where the virus may be spread by contaminated medical equipment, such as re-used needles. Sexual transmission of Lassa virus has been reported.
Lassa fever occurs in all age groups and both sexes. Persons at greatest risk are those living in rural areas where Mastomys are usually found, especially in communities with poor sanitation or crowded living conditions. Health workers are at risk if caring for Lassa fever patients in the absence of proper barrier nursing and infection prevention and control practices.
Diagnosis
Because the symptoms of Lassa fever are so varied and non-specific, clinical diagnosis is often difficult, especially early in the course of the disease. Lassa fever is difficult to distinguish from other viral haemorrhagic fevers such as Ebola virus disease as well as other diseases that cause fever, including malaria, shigellosis, typhoid fever and yellow fever.
Definitive diagnosis requires testing that is available only in reference laboratories. Laboratory specimens may be hazardous and must be handled with extreme care. Lassa virus infections can only be diagnosed definitively in the laboratory using the following tests:
- reverse transcriptase polymerase chain reaction (RT-PCR) assay
- antibody enzyme-linked immunosorbent assay (ELISA)
- antigen detection tests
- virus isolation by cell culture.
Treatment and prophylaxis
The antiviral drug ribavirin seems to be an effective treatment for Lassa fever if given early on in the course of clinical illness. There is no evidence to support the role of ribavirin as post-exposure prophylactic treatment for Lassa fever.
There is currently no vaccine that protects against Lassa fever.
Prevention and control
Prevention of Lassa fever relies on promoting good “community hygiene” to discourage rodents from entering homes. Effective measures include storing grain and other foodstuffs in rodent-proof containers, disposing of garbage far from the home, maintaining clean households and keeping cats. Because Mastomys are so abundant in endemic areas, it is not possible to completely eliminate them from the environment. Family members should always be careful to avoid contact with blood and body fluids while caring for sick persons.
In health-care settings, staff should always apply standard infection prevention and control precautions when caring for patients, regardless of their presumed diagnosis. These include basic hand hygiene, respiratory hygiene, use of personal protective equipment (to block splashes or other contact with infected materials), safe injection practices and safe burial practices.
Health-care workers caring for patients with suspected or confirmed Lassa fever should apply extra infection control measures to prevent contact with the patient’s blood and body fluids and contaminated surfaces or materials such as clothing and bedding. When in close contact (within 1 metre) of patients with Lassa fever, health-care workers should wear face protection (a face shield or a medical mask and goggles), a clean, non-sterile long-sleeved gown, and gloves (sterile gloves for some procedures).
Laboratory workers are also at risk. Samples taken from humans and animals for investigation of Lassa virus infection should be handled by trained staff and processed in suitably equipped laboratories under maximum biological containment conditions.
On rare occasions, travellers from areas where Lassa fever is endemic export the disease to other countries. Although malaria, typhoid fever, and many other tropical infections are much more common, the diagnosis of Lassa fever should be considered in febrile patients returning from West Africa, especially if they have had exposures in rural areas or hospitals in countries where Lassa fever is known to be endemic. Health-care workers seeing a patient suspected to have Lassa fever should immediately contact local and national experts for advice and to arrange for laboratory testing.
WHO response
The Ministries of Health of Guinea, Liberia and Sierra Leone, WHO, the Office of United States Foreign Disaster Assistance, the United Nations, and other partners have worked together to establish the Mano River Union Lassa Fever Network. The programme supports these 3 countries in developing national prevention strategies and enhancing laboratory diagnostics for Lassa fever and other dangerous diseases. Training in laboratory diagnosis, clinical management, and environmental control is also included.
An explosion tore through a train as it was traveling between two stations in St. Petersburg, Russia, killing at least 11 and injuring dozens more.
Monday, April 3rd, 2017Phase 2 Zika vaccine trial begins in U.S., Central and South America
Monday, April 3rd, 2017Friday, March 31, 2017
Study will evaluate NIH’s experimental DNA vaccine.
 A vial of the NIAID Zika Virus Investigational DNA Vaccine. NIAID
A vial of the NIAID Zika Virus Investigational DNA Vaccine. NIAIDVaccinations have begun in a multi-site Phase 2/2b clinical trial testing an experimental DNA vaccine designed to protect against disease caused by Zika infection. The vaccine was developed by government scientists at the National Institute of Allergy and Infectious Diseases (NIAID), part of the National Institutes of Health (NIH). NIAID is leading the trial, which aims to enroll at least 2,490 healthy participants in areas of confirmed or potential active mosquito-transmitted Zika infection, including the continental United States and Puerto Rico, Brazil, Peru, Costa Rica, Panama and Mexico. The two-part trial, called VRC 705, further evaluates the vaccine’s safety and ability to stimulate an immune response in participants, and assesses the optimal dose for administration. It also will attempt to determine if the vaccine can effectively prevent disease caused by Zika infection.
Most people with Zika infection have either no or only mild symptoms, such as fever, rash, joint pain and conjunctivitis (red eyes). However, when Zika infection occurs during pregnancy, the pregnant woman can pass the virus to her fetus, which can result in a range of fetal defects known collectively as congenital Zika syndrome. Currently there is no licensed vaccine to prevent disease caused by Zika infection, which is mainly transmitted via the bite of infected Aedes aegypti mosquitoes but also can be transmitted sexually.
“We are pleased to have advanced rapidly one of NIAID’s experimental Zika vaccines into this next stage of testing in volunteers. We expect this study will yield valuable insight into the vaccine’s safety and ability to prevent disease caused by Zika infection,” said NIAID Director Anthony S. Fauci, M.D. “A safe and effective Zika vaccine is urgently needed to prevent the often-devastating birth defects that can result from Zika virus infection during pregnancy. Evidence also is accumulating that Zika can cause a variety of health problems in adults as well. This trial marks a significant milestone in our efforts to develop countermeasures for a pandemic in progress.”
Scientists at NIAID’s Vaccine Research Center (VRC) developed the NIAID Zika virus investigational DNA vaccine. It entered early-stage human testing in 2016 following extensive testing in animal models. Initial findings indicate the vaccine is safe and able to induce a neutralizing antibody response against Zika virus. The Phase 2/2b trial aims to gain more safety and immune response data and determine if this immune response protects against disease caused by natural Zika infection.
The Zika vaccine platform is based on a strategy VRC scientists used previously to develop a West Nile virus vaccine candidate. The Zika vaccine candidate being tested in this study contains a small circular piece of DNA called a plasmid into which scientists have inserted genes that encode two proteins found on the surface of the Zika virus. Once injected into muscle, the encoded proteins assemble into particles that mimic Zika virus and trigger the body’s immune system to respond. The vaccine does not contain infectious material, so it cannot cause Zika infection.
The trial is being led by protocol co-chairs Julie E. Ledgerwood, D.O., chief of VRC’s Clinical Trials Program, and Grace L. Chen, M.D., deputy chief of the same program.
The trial consists of two studies: part A and part B. Part A will build on ongoing Phase 1 trials to further evaluate the vaccine’s safety and ability to stimulate an immune response, specifically in populations where Zika could be endemic. It will also help determine the optimal dose and injection sites for administration. Part A will enroll 90 healthy men and non-pregnant women ages 18-35 years at three sites in Houston, Miami and San Juan, Puerto Rico. All participants will receive the investigational vaccine intramuscularly at three separate clinic visits each four weeks apart. Participants will be randomly assigned to receive either a standard dose or a high dose of the investigational vaccine at all three visits, and will be followed for about 32 weeks total.
Part B of the trial will enroll at least 2,400 healthy men and non-pregnant women ages 15-35 years. This part of the trial aims to determine if the vaccine can effectively protect against Zika-related disease when someone is naturally exposed to the virus. Sites will include the three locations from part A (Houston, Miami and San Juan) as well as two additional sites in San Juan, two sites in Costa Rica, and one site each in Peru, Brazil, Panama and Mexico. Additional sites might be added in the future. Participants will be randomly assigned to receive either the investigational vaccine or a placebo at three separate clinic visits each four weeks apart. The trial is double-blind, meaning neither the study investigators nor the participants will know who receives the investigational vaccine.
Part B participants will be followed for nearly two years, during which time they will undergo assessments for adverse events and symptoms of Zika infection. Trial participants in both parts will be counseled on how to protect against Zika infection. Investigators will compare the rates of confirmed cases of Zika in the placebo group and the vaccinated group to determine if the investigational vaccine protects against disease caused by Zika infection.
Each site will have a principal investigator responsible for ensuring daily review of safety data as they become available. A protocol safety review team that includes the protocol chairs and other medical officers at NIAID will review safety data reports weekly. The NIAID Intramural Data and Safety Monitoring Board will also review cumulative study data at least twice per year. The study is currently expected to be completed by 2019.
For more information about the trial, visit Questions and Answers: VRC 705: Phase 2/2b Trial Testing the NIAID Zika Virus Investigational DNA Vaccine.
NIAID conducts and supports research — at NIH, throughout the United States, and worldwide — to study the causes of infectious and immune-mediated diseases, and to develop better means of preventing, diagnosing and treating these illnesses. News releases, fact sheets and other NIAID-related materials are available on the NIAID website.
About the National Institutes of Health (NIH): NIH, the nation’s medical research agency, includes 27 Institutes and Centers and is a component of the U.S. Department of Health and Human Services. NIH is the primary federal agency conducting and supporting basic, clinical, and translational medical research, and is investigating the causes, treatments, and cures for both common and rare diseases. For more information about NIH and its programs, visit www.nih.gov.
NIH…Turning Discovery Into Health®

4/2/1979: The world’s first anthrax epidemic begins in Sverdlosk, Russia. By the time it ended 6 weeks later, 62 were dead and another 32 survived serious illness.
Sunday, April 2nd, 2017https://www.youtube.com/watch?v=hi8vhbyt6r4