Archive for January, 2018
Human ectoparasites [(i.e. human fleas (Pulex irritans) or body lice (Pediculus humanus humanus)] were primary vectors for plague during the Second Pandemic, including the Black Death (1346–1353)
Wednesday, January 17th, 2018Human ectoparasites and the spread of plague in Europe during the Second Pandemic
PNAS 2018 : 1715640115v1-201715640.

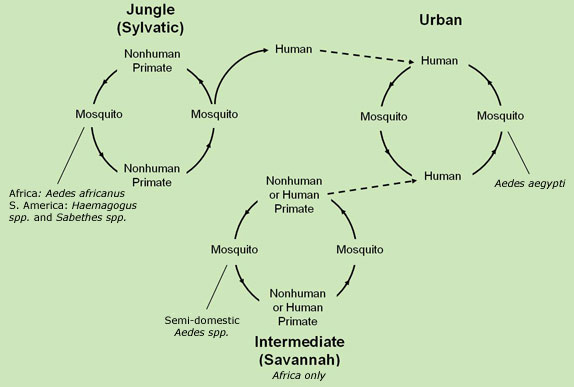
Between July of 2017 and the end of the year, there were 11 confirmed cases of yellow fever reported in Brazil, and since 2016, there have been 777 confirmed cases, 261 deaths.
Wednesday, January 17th, 2018“…..Between January 2016 and December 2017, seven countries and territories of the Region of the Americas reported confirmed cases of yellow fever: the Plurinational State of Bolivia, Brazil, Colombia, Ecuador, French Guiana, Peru, and Suriname….”

The Two-Finger Test: Rape survivors in India continue to be subjected to intrusive tests that the government and courts banned years ago
Tuesday, January 16th, 2018
A mezzanine floor has collapsed at the Jakarta stock exchange building (IDX), injuring dozens
Monday, January 15th, 20181/15/1919: Molasses burst from a huge tank flooding the streets of Boston, killing 21 people and injuring scores of others.
Monday, January 15th, 2018- A 58-foot-high tank filled with 2.5 million gallons of crude molasses.
- The bolts holding the bottom of the tank exploded, shooting out like bullets
- Hot molasses rushed out.
- An eight-foot-high wave of molasses swept away the freight cars and caved in the building’s doors and windows.
38 Minutes
Monday, January 15th, 2018“…..The Federal Communications Commission said on Sunday that its initial investigation of the mistaken alert had concluded that Hawaii did not have “reasonable safeguards or process controls in place” in its emergency notification process. The alert was sent to cellphones across Hawaii on Saturday morning when a state employee pushed the wrong button in the midst of a shift-change safety drill. It then took 38 minutes for the agency to withdraw the alert.
The prospect of a battery of investigations by state and federal lawmakers, with public testimony about the timeline of events, suggested that the alert would probably be a dominant subject in Hawaii life for months to come…..
As officials tried to reconstruct exactly what happened on Saturday, a spokesman for the Pacific Command in Hawaii said the military had moved quickly to push back against the Hawaii state alert as soon as it was known to be incorrect.
“Upon confirming yesterday’s message was a false alarm, Uspacom Public Affairs worked quickly to inform the public through traditional and social media channels,” Cmdr. David Benham, a military spokesman, said in an email Sunday, using an acronym for the Pacific Command. “We will use this as an opportunity to improve our internal processes as well as coordination with State authorities. “
The Pacific Command first told Hawaii media that there was no approaching ballistic missile at 8:23 a.m. — about 13 minutes after Hawaii sent out the alert………”

Tainted sea turtles allegedly killed 10 Madagascaris including a 1-year old.
Monday, January 15th, 2018Translation: “….After returning from
fishing, the villagers divided the meat from 2 sea turtles.
Immediately after the meal the 1st symptoms of food poisoning
appeared. People could not stop vomiting and were taken to hospital.
In spite of intensive care of the ill, 10 people, including a baby of
one year, did not survive…..”


One or two dead & 65 injured in 7.1-magnitude Peru earthquake
Monday, January 15th, 2018https://www.youtube.com/watch?v=H0GVP0sf3wE
The Philippines’ most active volcano, Mayon, has shown signs of imminent eruption, forcing thousands of people on the main island of Luzon to evacuate.
Monday, January 15th, 2018Bill Gates at J.P. Morgan’s 36th Annual Healthcare Conference
Monday, January 15th, 2018The business of improving global health
Some of the world’s most debilitating diseases are treated by a medication that was originally created for dogs.
It sounds weird, but it’s true. In 1978, a researcher at Merck hypothesized that a new heartworm preventative called ivermectin could help people suffering from onchocerciasis, a neglected tropical disease that causes river blindness primarily in sub-Saharan Africa. Less than a decade later, the drug was approved for use in humans, and Merck announced that it would provide ivermectin for free to anyone who needs it.
Today, it’s used to treat people suffering from a number of parasitic diseases. I recently saw firsthand how the Tanzanian government is administering ivermectin to whole communities to wipe out lymphatic filariasis.
The next ivermectin could be sitting in a lab right now, but we need to be purposeful about finding it. Private sector research can have tremendous benefits for the world’s poorest. If you look at the research agendas of many biotech and pharma companies today, I think there are enormous opportunities to make progress on some of the toughest health challenges.
I spoke about the possibilities that exist at the intersection of global health and the private sector earlier today at J.P. Morgan’s 36th Annual Healthcare Conference in San Francisco. Here is the full text of my prepared remarks:
Remarks as prepared
J.P. Morgan’s 36th Annual Healthcare Conference
San Francisco, CA
January 8, 2018
BILL GATES:
Thank you. It’s great to be here today.
No matter where I go, no matter who I talk to, there’s one point I always try to get across. It’s been my key message for more than a decade. It’s that health is getting better, and it’s getting better faster than ever before.
Since 1990, the world has cut child mortality in half. HIV is no longer a certain death sentence. Many of the so-called neglected diseases that affect a billion people every year aren’t neglected anymore.
I talk about what we’ve accomplished in the past because it makes me optimistic about what we can accomplish in the future. But there’s still a lot of room for improvement. This year, 5 million children under the age of five will die, mostly in poor countries. And hundreds of millions of others will suffer from diseases and malnutrition that sap them, and their countries, of their strength and their potential.
Some of this can be addressed by doing a better job of getting lifesaving drugs and vaccines to the people who need them. But there is still a substantial gap between the tools we have and the tools we need to eliminate the most persistent diseases of poverty.
The way to fill that gap is to innovate, and that’s why I’m excited to be here today. Because the tools and discoveries your companies are working on can also lead to breakthrough solutions that save millions of lives in the world’s poorest countries.
It’s true that government-funded basic science research shines a light on promising pathways to health advances.
Philanthropy can help nurture the best ideas through discovery and development, and balance the risk-reward equation for private-sector partners.
But industry has the skills, experience, and capacity necessary to turn discoveries into commercially viable products.
The fact is that global health needs the private sector. And, frankly, the private sector has much to gain from pursuing breakthroughs in global health.
Over the next few decades, developing economies will continue to expand. By 2050, the population of Africa will more than double to almost 2.5 billion. That’s more than twice the forecasted population of the U.S. and Europe combined.
But we don’t have to wait 20 or 30 years. Even in the shorter term, impact and earnings are not mutually exclusive for the private-sector.
As you probably know, global health is our primary focus at the Gates Foundation—although we also work in a few other areas that are big levers for impact . . . like agricultural development . . . and public education here in the U.S. Over the last five years, we have invested nearly $12 billion in global health.
This includes grants and equity investments in companies with promising technologies that have potential application in global health. We also use creative price and volume guarantees that help the private sector mitigate the risk in developing a new product for which demand is unproven.
Our investments have led to new drugs and vector control tools for malaria . . . accelerated the introduction of new vaccines in poor countries . . . and ensured that millions of people in the developing world have access to long-lasting contraceptives and the best-available antiretroviral treatment for HIV.
We are also working with the WHO and regulatory entities in China and Africa to eliminate systemic barriers that slow development of new products and access to new markets. A few years ago, we looked at the data, which showed that in high-income countries it took 6-12 months to get a product registered—compared to 4-7 years in low-income countries. We realized this was as big a challenge as anything else in getting new health solutions to the people who need them.
I’m particularly excited about our work with the Chinese FDA to provide a more efficient and consistent mechanism for testing, review, and approval of medicines and vaccines—using international standards. This would be a game changer in getting quality products into and out of China.
There is another critical intersection emerging between what you do and what we do—and that’s what I’d like to talk about today.
The questions driving your research agendas today in biotech and pharma—and the problems we’re trying to solve in global health—are starting to converge in exciting ways. Many of the solutions you’re working on—harnessing the immune system to tackle cancer, unraveling the mysteries of the brain to treat Alzheimer’s, and learning how bodies absorb nutrition to address the obesity epidemic and other diseases—also have clear applications in global health.
The global health community may not be thinking as much about treatments for cancer, but we need to understand the immune system to tackle deadly diseases like HIV, malaria, and TB.
We aren’t focused on the neurodegenerative diseases commonly associated with aging, but we are concerned about the cognitive development of hundreds of millions of young children in poor countries.
We aren’t dealing with a crisis of obesity in Africa and South Asia, but we are trying to address its inverse, a crisis of stunting, wasting, and undernutrition.
You may be interested in developing products for rich-world markets, but the breakthroughs happening in your labs can also save millions of lives in the world’s poorest countries.
In health and medicine, we learn by analogy. We borrow insights from other fields. And when we ask one kind of question about key systems like the immune system, the brain, or our human microbiota, the answers may also apply to a totally different line of questioning.
A few months ago, a headline caught my eye in The Wall Street Journal. The story was one of many that have highlighted how the HIV virus’s genetic machinery can be used as a tool to modify T-cells so they are capable of attacking specific cancers.
I’m confident that a decade from now, we’ll see a headline that says: “How Cancer Tools are Helping Cure HIV.”
Of course, it’s not quite that simple. Immunotherapy today works only against certain types of cancers and only in certain patients. And, like cancer, infectious diseases such as HIV, TB, and malaria have complex interactions with the immune system of infected individuals.
But there is reason to hope that the insights uncovered in ongoing immunotherapy research for cancer will eventually help us control all infectious diseases. This would be a huge victory for humanity—and potentially a significant market for the life sciences.
Others seem to think so too. Venture capitalists like Bob Nelsen and Bob More have helped raise over $500 million for VIR Biotechnology—including funding from us—to discover and develop treatments for serious infectious diseases.
We are also investors in Immunocore, which is using T-cell technology to help stimulate the body’s immune system. Initially, Immunocore’s “T-cell receptor” technology targeted cancers, but it could also be applied against infectious diseases.
We are backing companies like CureVac and Moderna on mRNA approaches for vaccine and drug development, which have the potential to help us tackle cancer. This approach is also intriguing as a potential immunological intervention for HIV, malaria, flu and the Zika virus.
And mRNA vaccines are likely to be cheaper, easier, and faster to make than traditional vaccines. This would be particularly helpful in containing epidemics—whether they occur through nature or are the result of an intentional biological attack. Today, it typically takes up to 10 years to develop and license a new vaccine. To significantly curb deaths from a fast-moving airborne pathogen, we would have to get that down considerably—to 90 days or less.
Of course, fighting infectious disease is only one of the global health challenges that demand our attention. Another is newborn health. Despite the great progress in reducing child mortality, nearly 5 million children under the age of five will die this year—close to half in the first 28 days of life.
To make inroads against neonatal mortality, we first have to understand and address the underlying vulnerabilities of newborns, especially in poor countries. Right now, we don’t know exactly why many newborns in poor countries die, which makes it very difficult to save them.
But we’re enthusiastic about leveraging the tools of genetics and other research the private sector is working on to help children survive birth, fend off deadly infections, and thrive both physically and cognitively.
I’m also excited about a 20-year study we’re funding in Southeast Asia and Sub Saharan Africa that will give us epidemiological data about what is causing stillbirths and child deaths.
We have a lot to learn from the data, but we already know that one critical factor is the prevalence of preterm birth. It is the single largest cause of newborn deaths, and the children who survive it often face serious and lifelong health problems. Although most premature births occur in Africa and Asia, this remains a problem in rich countries, too.
One of every 10 infants in the U.S. is born preterm, which threatens the health and wellbeing of those children and significantly drives up healthcare costs.
We are just now getting the first effective diagnostic test to identify women at risk for early delivery. A company called Sera Prognostics developed a blood-based diagnostic that recently went on the market in the U.S.
We’re supporting their work on a low-cost version for use in poor countries. By itself, this won’t solve the problem. But it will give healthcare providers a way to identify women at risk and provide care that extends their pregnancy toward full-term.
We also need to better understand the biological mechanisms that underpin preterm birth, starting with the health of the mother during pregnancy. We recently co-funded a genome wide association study that illuminated a correlation between selenium deficiency in pregnant women and preterm birth. More research is needed, but the hope is that dietary supplements could help reduce the incidence of preterm births and newborn deaths.
It is also increasingly clear that the gut microbiome and nutrition—and the interplay between the two—is a big factor in the survival and healthy development of children, no matter where they live.
We know that children in poor countries who are malnourished and vulnerable to enteric infections have underdeveloped microbiomes that weaken their immune system and make them more susceptible to disease and to impaired brain development that lasts a lifetime.
There is also evidence that children in wealthy countries who grow up in super-hygienic environments—with an abundance of processed foods and antibiotics—have poor gut health that makes them more susceptible to obesity, auto-immune diseases, diabetes—and later in life—hypertension.
The solution in both instances is making sure that kids have the right constellation of microbes in their gut—and that they’re eating the right foods to support a healthy microbiome.
We’ve recently begun working with partners who are developing solutions to replace or augment healthy microbes using probiotics, nutritious foods with locally-available ingredients, and even fecal transplants.
We also have to better understand which children are not progressing developmentally, and why that is.
As I mentioned, malnourished children are at risk of being cognitively impaired for the rest of their lives. Recent estimates indicate that 250 million children under the age of five fit this criterion. That’s four of every 10 children in low- and middle-income countries who are more likely to drop out of school and less likely to succeed in the workplace.
In human terms, this is a heartbreaking tragedy. In economic terms, it is a huge drag on the ability of developing countries to lift themselves out of poverty.
One challenge is that we don’t have good tools to assess the brain development of children. The proxy measures we use today are a child’s height—if it’s well below the norm for their age—and whether they live in poverty. There is, of course, value in these indicators. But we can’t adequately gauge the development of an organ that contains 100 billion cells and that scientists have called “the most complex object in the known universe” through measures that are apparent to the naked eye.
We are working with partners to determine if neuroimaging and other technologies can be used in early infancy and young children to accurately predict cognitive development. These are the same tools that companies are using to assess dementia and cognitive decline late in life.
We have some early data showing the promise of these tools in parts of the world with a high incidence of stunting. These images show fewer neural connections in the brains of children who are stunted compared to the brains of normally developing children at 2-3 months of age.
We’re also supporting research to better understand the factors that most affect brain development in children so we can intervene more quickly to minimize the impact of neurocognitive deficits early in life.
On a personal level, I’m particularly interested in deepening our understanding of both the development and the decline of brain function.
I’ve seen first-hand the devastating consequences of stunting on the development of children in developing countries. And men in my own family have suffered from Alzheimer’s.
Although Alzheimer’s research is outside the scope of what we do as a foundation, I’ve personally committed to investing $100 million on new approaches to dementia, including Alzheimer’s—on top of the brain development research we’re supporting through the foundation.
People often ask why Melinda and I decided to focus so much of our philanthropy on global health. It started with a simple question we asked ourselves: how could we do the most good for the greatest number of people?
When we looked at it that way, the answer quickly became clear. The health disparity between rich and poor countries was a big problem. We saw a gap that wasn’t being filled by others. And we believed that our investments in global health could be catalytic. By helping poor countries ease the devastating burden of disease, we could help ease the burden of poverty, too.
One of the major obstacles we faced early on is that in health—as in many other aspects of life—the free market tends to work well for people who can pay . . . and not so well for people who can’t. But over the last decade, our experience has shown that we can stretch the reach of market forces so the private sector’s most exciting innovations also benefit people with the most urgent needs. And with creative thinking, we can do it in ways that are both sustainable and profitable.
Our foundation is in a unique position to share the risk on promising bets that can lead to important new discoveries. And we can help provide more predictability to companies interested in entering new markets that present real challenges—but also tremendous opportunities.
We all share the goal of improving the health and well-being of people globally. Imagine what’s possible if we work together.
Consider a world where the age-old scourge of malaria is finally eradicated . . . where hundreds of millions of people no longer suffer from tuberculosis . . . and where we have a cure for HIV.
In a quarter century, we cut childhood mortality in half. With the passion, expertise, and resources of the people in this room, we can cut child mortality in half again by 2030.
There are many technical challenges to overcome. But when I think about the breathtaking pace of innovation in just the last 10 or 20 years, I believe that even more extraordinary things are possible in our lifetime.
I can think of no more noble purpose than erasing the divide between those who suffer the relentlessness of disease and poverty—and those of us who enjoy good health and prosperity.
Achieving health equity in our lifetime is not only a possibility. It is an imperative, because everyone—no matter where they live—deserves the chance to live a healthy and productive life.
Thank you.