Archive for March, 2018
WHO: List of Blueprint priority diseases
Sunday, March 11th, 2018List of Blueprint priority diseases

2018 annual review of the Blueprint list of priority diseases
For the purposes of the R&D Blueprint, WHO has developed a special tool for determining which diseases and pathogens to prioritize for research and development in public health emergency contexts. This tool seeks to identify those diseases that pose a public health risk because of their epidemic potential and for which there are no, or insufficient, countermeasures. The diseases identified through this process are the focus of the work of R& D Blueprint. This is not an exhaustive list, nor does it indicate the most likely causes of the next epidemic.
The first list of prioritized diseases was released in December 2015.
Using a published prioritization methodology, the list was first reviewed in January 2017.
The second annual review occurred 6-7 February, 2018. Experts consider that given their potential to cause a public health emergency and the absence of efficacious drugs and/or vaccines, there is an urgent need for accelerated research and development for*:
- Crimean-Congo haemorrhagic fever (CCHF)
- Ebola virus disease and Marburg virus disease
- Lassa fever
- Middle East respiratory syndrome coronavirus (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS)
- Nipah and henipaviral diseases
- Rift Valley fever (RVF)
- Zika
- Disease X
Disease X represents the knowledge that a serious international epidemic could be caused by a pathogen currently unknown to cause human disease, and so the R&D Blueprint explicitly seeks to enable cross-cutting R&D preparedness that is also relevant for an unknown “Disease X” as far as possible.
A number of additional diseases were discussed and considered for inclusion in the priority list, including: Arenaviral hemorrhagic fevers other than Lassa Fever; Chikungunya; highly pathogenic coronaviral diseases other than MERS and SARS; emergent non-polio enteroviruses (including EV71, D68); and Severe Fever with Thrombocytopenia Syndrome (SFTS).
These diseases pose major public health risks and further research and development is needed, including surveillance and diagnostics. They should be watched carefully and considered again at the next annual review. Efforts in the interim to understand and mitigate them are encouraged.
Although not included on the list of diseases to be considered at the meeting, monkeypox and leptospirosis were discussed and experts stressed the risks they pose to public health. There was agreement on the need for: rapid evaluation of available potential countermeasures; the establishment of more comprehensive surveillance and diagnostics; and accelerated research and development and public health action.
Several diseases were determined to be outside of the current scope of the Blueprint: dengue, yellow fever, HIV/AIDs, tuberculosis, malaria, influenza causing severe human disease, smallpox, cholera, leishmaniasis, West Nile Virus and plague. These diseases continue to pose major public health problems and further research and development is needed through existing major disease control initiatives, extensive R&D pipelines, existing funding streams, or established regulatory pathways for improved interventions. In particular, experts recognized the need for improved diagnostics and vaccines for pneumonic plague and additional support for more effective therapeutics against leishmaniasis.
The experts also noted that:
- For many of the diseases discussed, as well as many other diseases with the potential to cause a public health emergency, there is a need for better diagnostics.
- Existing drugs and vaccines need further improvement for several of the diseases considered but not included in the priority list.
- Any type of pathogen could be prioritised under the Blueprint, not only viruses.
- Necessary research includes basic/fundamental and characterization research as well as epidemiological, entomological or multidisciplinary studies, or further elucidation of transmission routes, as well as social science research.
- There is a need to assess the value, where possible, of developing countermeasures for multiple diseases or for families of pathogens.
The impact of environmental issues on diseases with the potential to cause public health emergencies was discussed. This may need to be considered as part of future reviews.
The importance of the diseases discussed was considered for special populations, such as refugees, internally displaced populations, and victims of disasters.
The value of a One Health approach was stressed, including a parallel prioritization processes for animal health. Such an effort would support research and development to prevent and control animal diseases minimising spill-over and enhancing food security. The possible utility of animal vaccines for preventing public health emergencies was also noted.
Also there are concerted efforts to address anti-microbial resistance through specific international initiatives. The possibility was not excluded that, in the future, a resistant pathogen might emerge and appropriately be prioritized.
*The order of diseases on this list does not denote any ranking of priority.
Disease X: A pathogen with the potential to spread and kill millions but for which there are currently no, or insufficient, countermeasures available.
Sunday, March 11th, 2018“……It was the third time the committee, consisting of leading virologists, bacteriologists and infectious disease experts, had met to consider diseases with epidemic or pandemic potential. But when the 2018 list was released two weeks ago it included an entry not seen in previous years.
- Crimean-Congo haemorrhagic fever (CCHF)
- Ebola virus disease and Marburg virus disease
- Lassa fever
- Middle East respiratory syndrome coronavirus (MERS-CoV) and Severe Acute Respiratory Syndrome (SARS)
- Nipah and henipaviral diseases
- Rift Valley fever (RVF)
- Zika
- Disease X
*Diseases posing significant risk of an international public health emergency for which there is no, or insufficient, countermeasures. Source: World Health Organization (WHO), 2018
CDC: influenza-like illness (ILI) activity is markedly down across the country this week, a clear sign that this year’s severe flu season continues to wind down.
Friday, March 9th, 2018Synopsis:
During week 9 (February 25-March 3, 2018), influenza activity decreased in the United States.
- Viral Surveillance: Overall, influenza A(H3) viruses have predominated this season. However, in recent weeks the proportion of influenza A viruses has declined, and during week 9, the numbers of influenza A and influenza B viruses reported were similar. The percentage of respiratory specimens testing positive for influenza in clinical laboratories decreased.
- Pneumonia and Influenza Mortality: The proportion of deaths attributed to pneumonia and influenza (P&I) was above the system-specific epidemic threshold in the National Center for Health Statistics (NCHS) Mortality Surveillance System.
- Influenza-associated Pediatric Deaths: Five influenza-associated pediatric deaths were reported.
- Influenza-associated Hospitalizations: A cumulative rate of 86.3 laboratory-confirmed influenza-associated hospitalizations per 100,000 population was reported.
- Outpatient Illness Surveillance:The proportion of outpatient visits for influenza-like illness (ILI) was 3.7%, which is above the national baseline of 2.2%. All 10 regions reported ILI at or above region-specific baseline levels. New York City and 21 states experienced high ILI activity; 15 states experienced moderate ILI activity; the District of Columbia, Puerto Rico, and five states experienced low ILI activity; and nine states experienced minimal ILI activity.
- Geographic Spread of Influenza:The geographic spread of influenza in Puerto Rico and 34 states was reported as widespread; Guam and 12 states reported regional activity; the District of Columbia and four states reported local activity; and the U.S. Virgin Islands reported no activity.

In the first chaotic moments after a gunman opened fire at Marjory Stoneman Douglas High School in Parkland, Fla., 81 people called 911 desperate for help.
Friday, March 9th, 2018“…..The office released recordings of 10 calls that sometimes depict panicked parents furiously texting their children at the school and relaying information to law enforcement.….”
Security Alert – U. S. Embassy Mexico City, Mexico (March 7, 2018)
Friday, March 9th, 2018Location: Playa del Carmen, Mexico
Event: On March 7, the U.S. Embassy in Mexico City received information about a security threat in Playa del Carmen, Quintana Roo, Mexico. Effective immediately, U.S. Government employees are prohibited from traveling to Playa del Carmen until further notice. The U.S. Consular Agency in Playa del Carmen will be closed until further notice.
Actions to Take:
- Be aware of your surroundings and exercise caution.
- Purchase travel insurance that specifically covers you in Mexico and includes medical evacuation insurance.
- Contact the nearest U.S. Embassy or Consulate if you need assistance.
Assistance:
U.S. Embassy Mexico City, Mexico
(011-52-55) 5080-2000
ACSMexicoCity@state.gov
https://mx.usembassy.gov/embassy-consulates/
State Department – Consular Affairs
888-407-4747 or 202-501-4444
- Mexico Country Information
- Enroll in Smart Traveler Enrollment Program (STEP) to receive security updates
- Follow us on Facebook and Twitter
After a nerve-agent attack on an ex-Russian spy, “around 21” had been given medical help and support
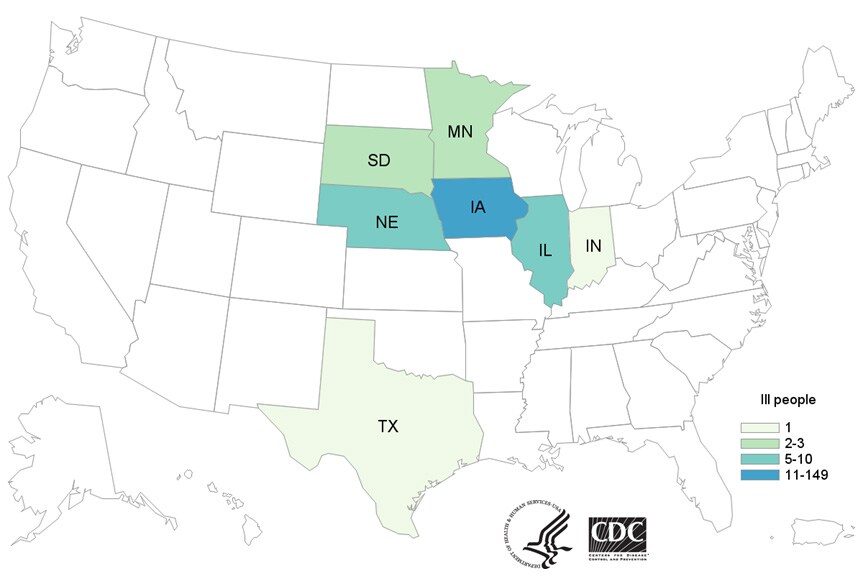
Friday, March 9th, 2018Multistate Outbreak of Salmonella Typhimurium Linked to Chicken Salad
Friday, March 9th, 2018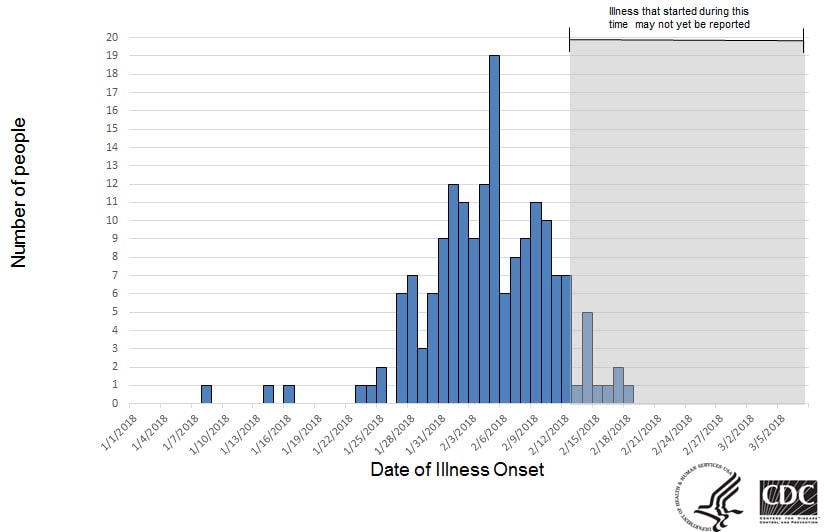
Saudi MOH: Another MERS-CoV case in a presumed hospital-based outbreak that has included 3 other patients and 1 healthcare provider
Friday, March 9th, 2018
The Model Uniform Core Criteria for Mass Casualty Incident Triage
Friday, March 9th, 2018The Model Uniform Core Criteria for Mass Casualty Incident Triage, or MUCC, is a standard set of guidelines that all mass casualty triage systems should follow. The MUCC is intended to ensure consistency among responders when triaging patients at a mass casualty incident. The SALT Triage System is the only triage method which currently meets the Model Uniform Core Criteria.