Archive for April, 2018
CDC: Multistate Outbreak of E. coli O157:H7 Infections Linked to Chopped Romaine Lettuce
Saturday, April 14th, 2018Case Count Update
Since the last update on April 10, 2018, 18 more people from 9 states were added to this outbreak.
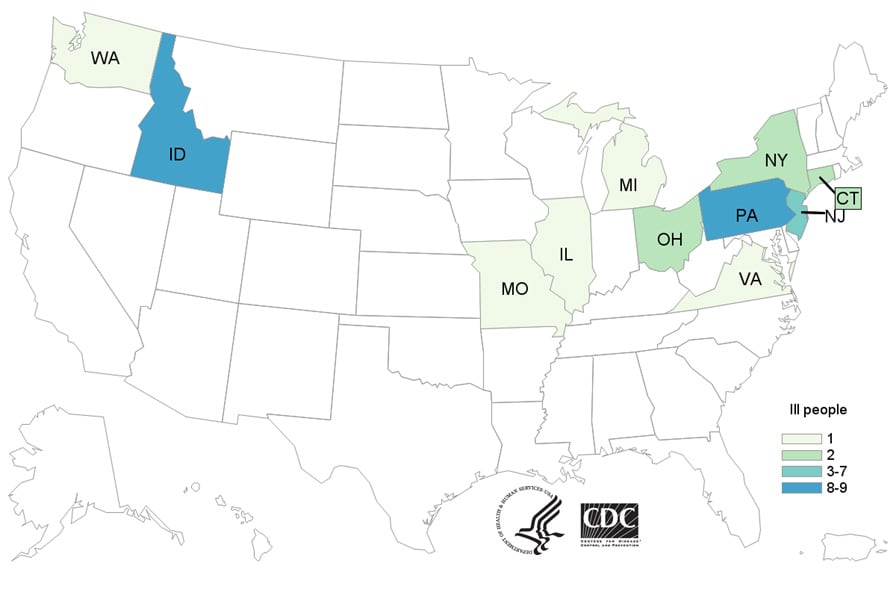
As of April 12, 2018, 35 people infected with the outbreak strain of E. coli O157:H7 have been reported from 11 states. A list of the states and the number of cases in each can be found on the Case Count Map page. Illnesses started on dates ranging from March 22, 2018 to March 31, 2018. Ill people range in age from 12 to 84 years, with a median age of 29. Sixty-nine percent of ill people are female. Twenty-two ill people have been hospitalized, including three people who developed hemolytic uremic syndrome, a type of kidney failure. No deaths have been reported.
Illnesses that occurred after March 27, 2018, might not yet be reported due to the time it takes between when a person becomes ill with E. coli and when the illness is reported. This takes an average of two to three weeks.
The current outbreak is not related to a recent multistate outbreak of E. coli O157:H7 infections linked to leafy greens. People in the previous outbreak were infected with a different DNA fingerprint of E. coli O157:H7 bacteria.
Investigation Update
Epidemiologic evidence collected to date indicates that chopped romaine lettuce is the likely source of this outbreak. Twenty-six (93%) of 28 people interviewed reported consuming romaine lettuce in the week before their illness started. This percentage is significantly higher than results from a survey[787 KB] of healthy people in which 46% reported eating romaine lettuce in the week before they were interviewed. Most people reported eating a salad at a restaurant, and romaine lettuce was the only common ingredient identified among the salads eaten. The restaurants reported using bagged, chopped romaine lettuce to make salads. At this time, ill people are not reporting whole heads or hearts of romaine.
Traceback investigations are ongoing to determine the source of chopped romaine lettuce supplied to restaurant locations where ill people ate. At this time, no common grower, supplier, distributor, or brand has been identified. However, preliminary information indicates that the chopped romaine lettuce was from the Yuma, Arizona growing region.
Information collected to date indicates that chopped romaine lettuce from the Yuma, Arizona growing region could be contaminated with E. coli O157:H7 and could make people sick. Read CDC’s advice to consumers, restaurants, and retailers.
This investigation is ongoing, and CDC will provide more information as it becomes available.
The Director of the Environmental Health Office in Zliten confirmed that the recorded cases of leishmaniasis this year has increased to 51 persons in the city.
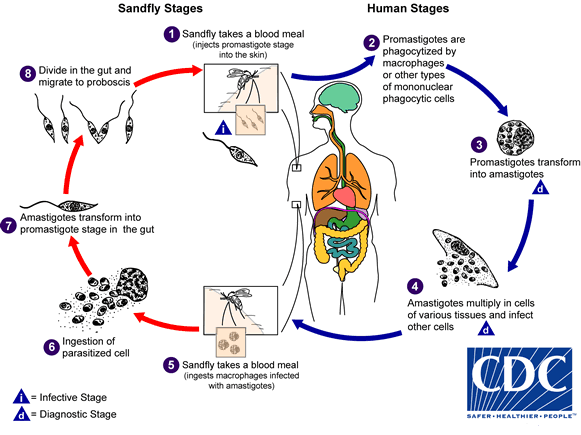
Saturday, April 14th, 2018“….[He] explained that there is no cure at the current time for the disease in Libya, noting that the cost of treatment for this disease is prohibitively expensive and could amount to 10 thousand Libyan dinars per person….. Zliten Municipality warned against the spread of leishmaniasis, declaring that 351 cases were recorded in the city in 2017…..Leishmaniasis is a parasitic disease spread to humans by bites of sandflies that are usually active from May to September each year…..”
 Credit: C. Bern, CDC
Credit: C. Bern, CDC
 (Credit: B. Arana, MERTU, Guatemala)
(Credit: B. Arana, MERTU, Guatemala)


4/13/1919: In Amritsar, India’s holy city of the Sikh religion, British and Gurkha troops massacre at least 379 unarmed demonstrators
Friday, April 13th, 2018Testing by four laboratories affiliated with The Organization for the Prohibition of Chemical Weapons have confirmed British findings on the nerve agent used in last month’s attack on a former Russian spy in England
Friday, April 13th, 2018“….There are several variants of Novichok, a binary weapon containing two less toxic chemicals that, when mixed, react to produce a poison several times more lethal than sarin or VX.
Russia’s ambassador to Britain, Alexander Yakovenko, has identified the alleged poison as Novichok A-234, derived from an earlier version known as A-232…..”
THE HAGUE, Netherlands — 12 April 2018 — “The Organisation for the Prohibition of Chemical Weapons (OPCW) transmitted yesterday to the United Kingdom of Great Britain and Northern Ireland (UK) the report of the OPCW’s mission to provide requested technical assistance in regard to the Salisbury incident on 4 March 2018.
The results of the analysis by the OPCW designated laboratories of environmental and biomedical samples collected by the OPCW team confirm the findings of the United Kingdom relating to the identity of the toxic chemical that was used in Salisbury and severely injured three people.
The UK’s delegation to the OPCW requested that the Technical Secretariat share the report with all States Parties to the Chemical Weapons Convention (CWC) and to make the Executive Summary of the report publicly available.
The Director-General, Ambassador Ahmet Üzümcü, thanked the four OPCW designated laboratories that supported the technical assistance request for their swift and thorough analysis.
Background
The United Kingdom of Great Britain and Northern Ireland requested technical assistance from the OPCW Technical Secretariat, under subparagraph 38(e) of Article VIII of the Chemical Weapons Convention, in relation to an incident in Salisbury on 4 March 2018 involving a toxic chemical—allegedly a nerve agent—and the poisoning and hospitalisation of three individuals.
The OPCW team worked independently and is not involved in the national investigation by the UK authorities. No State Party was involved in the technical work carried out by the Technical Secretariat.
OPCW designated laboratories are a lynchpin of the Organisation’s verification regime and its capacity to investigate allegations of the use of chemical weapons. They must be able to perform off-site analysis of chemical samples collected by OPCW inspectors from chemical production facilities, storage depots and other installations, or from the site of an alleged use of chemical weapons. These laboratories offer the necessary assurance to our States Parties that chemical analyses needed to make determinations or to clarify issues occurring during OPCW deployments are carried out competently, impartially, and with unambiguous results.
As the implementing body for the Chemical Weapons Convention, the OPCW oversees the global endeavour to permanently and verifiably eliminate chemical weapons. Since the Convention’s entry into force in 1997 – and with its 192 States Parties – it is the most successful disarmament treaty eliminating an entire class of weapons of mass destruction.
Over ninety-six per cent of all chemical weapon stockpiles declared by possessor States have been destroyed under OPCW verification. For its extensive efforts in eliminating chemical weapons, the OPCW received the 2013 Nobel Prize for Peace.”
More Information
University of Iowa study: A vaccination used to treat dogs with leishmaniasis could be effective in containing its spread to humans.
Friday, April 13th, 2018“….Leishmaniasis is a tropical infectious disease found in 98 countries around the globe. According to an estimate from the World Health Organization, it kills approximately 20,000 to 40,000 people a year in mostly five countries: Bangladesh, Brazil, Ethiopia, India, and Sudan. It also kills thousands of dogs.….”
Nearly one billion people will be vaccinated against yellow fever in 27 high-risk African countries by 2026 with support from WHO, Gavi – the Vaccine Alliance, UNICEF and more than 50 health partners.
Thursday, April 12th, 201810 April 2018 | Abuja, Nigeria – Nearly one billion people will be vaccinated against yellow fever in 27 high-risk African countries by 2026 with support from WHO, Gavi – the Vaccine Alliance, UNICEF and more than 50 health partners.
The commitment is part of the Eliminate Yellow fever Epidemics (EYE) in Africa strategy, which was launched by Dr Tedros Adhanom Ghebreyesus, WHO Director-General, Professor Isaac Folorunso Adewole, Nigeria’s Minister of Health and partners at a regional meeting in Abuja, Nigeria on Tuesday (10 April).

“The world is facing an increased risk of Yellow fever outbreaks and Africa is particularly vulnerable,” said Dr Tedros. “With one injection we can protect a person for life against this dangerous pathogen. This unprecedented commitment by countries will ensure that by 2026 Africa is free of Yellow fever epidemics.”
During the three-day EYE strategy regional launch meeting representatives from key African countries, WHO, UNICEF, Gavi, and other partners are developing a roadmap on how to roll-out the EYE strategy at national level. This implementation effort follows the endorsement of the strategy by African Ministers of Health at the 67th WHO regional committee in September 2017.
“This comprehensive, global strategy offers an unprecedented opportunity to end the devastating Yellow fever epidemics that periodically impact Africa,” said Dr Seth Berkley, CEO of Gavi, the Vaccine Alliance. “Ensuring that the most vulnerable communities have access to the vaccine through routine systems plays a central role in making this happen. Vaccine manufacturers and Gavi partners have worked hard to improve the global vaccine supply situation in recent years to make sure there is enough vaccine to respond to outbreaks, allow preventive campaigns and that routine immunization functions at full capacity.”
The three objectives of the strategy include protecting at-risk populations through preventive mass vaccination campaigns and routine immunization programmes, preventing international spread, and containing outbreaks rapidly. Developing strong surveillance with robust laboratory networks is key to these efforts.
UNICEF will make vaccines available, advocate for greater political commitment and provide support in vaccinating children through routine immunization as well as during outbreaks of the disease.
“Today, the threat of yellow fever looms larger than ever before, especially for thousands of children across Africa,” said Stefan Peterson, UNICEF’s Chief of Health. “Given that almost half of the people to be vaccinated are children under 15 years of age, this campaign is critical to saving children’s lives, and would go a long way toward stamping out this disease.”
After outbreaks of Yellow fever in densely populated cities in Angola and the Democratic Republic of Congo caused 400 deaths in 2016, the acute viral haemorrhagic disease re-emerged as a serious global public health threat. Brazil is currently battling its worst outbreak of Yellow fever in decades with more than 1,000 confirmed cases. The ease and speed of population movements, rapid urbanization and a resurgence of mosquitoes due to global warming have significantly increased the risk of urban outbreaks with international spread.
Experience in West Africa demonstrates that the EYE strategy can work. When Yellow fever re-emerged as a public health issue in the early 2000s, countries in the region controlled the epidemics through preventive mass campaigns combined with routine immunization. No yellow fever epidemics have been recorded since in countries which successfully implemented this approach.
Note to the Editors
The EYE strategy partners include GAVI the Vaccine Alliance, Endemic and New Technologies Franchise Sanofi Pasteur, Sealy Center for Vaccine Development at the University of Texas, GE Foundation, United Nations Children’s Fund (UNICEF), United States Agency for International Development (USAID), Agence de Médecine Préventive (AMP), School of Veterinary Medicine University of Surrey, Bio Manguinhos/Fiocruz, Department for International Development (DFID), Institut Pasteur Dakar, ExxonMobil, Save the Children, ArcelorMittal, Wellcome Trust, Imperial College London, Centers for Disease Control and Prevention (CDC), United Nations High Commissioner for Refugees (UNHCR), Sanofi Pasteur, Department of Tropical Medicine University of Hawaii, Medair, Chumakov Federal Scientific Center for Research & Development of Immune-and-Biological Products Russian Academy of Medical Sciences, China National Biotech Group, Skoll Global Threats Fund, Bill & Melinda Gates Foundation, International Federation of Red Cross and Red Crescent Societies (IFRC), National Institutes of Health (NIH), BioProtection Systems/NewLikn Genetics Corp., Robert Koch-Institut, Regional Immunization Technical Advisory Group (RITAG), PATH – Center for Vaccine Innovation and Access, Department of Entomology University of California, World Meteorological Organization (WMO), Vaccinology and Immunology Unit University Hospitals Geneva, Nigerian Academy of Science, Médecins Sans Frontières (MSF), Instituto Evandro Chagas (IEC), International Organization for Migration (IOM) and European Centre for Disease Prevention and Control (ECDC).
San Diego, CA: Three recent wound botulism cases are linked to black tar heroin use
Thursday, April 12th, 2018“……They were hospitalized after experiencing a range of symptoms including double vision, drooping eyelids, difficulty swallowing, slurred speech and generalized weakness.
All three have required intensive care treatment with an anti-toxin that counteracts the effects of a neurotoxin produced by clostridium botulinum….”
The largest patient movement exercise in U.S. Department of Health and Human Services’ history began 4/10/18 to test the nationwide ability to move patients with highly infectious diseases safely and securely to regional treatment centers.
Thursday, April 12th, 2018HHS sponsors its largest exercise for moving patients with highly infectious diseases
The largest patient movement exercise in U.S. Department of Health and Human Services’ history began today to test the nationwide ability to move patients with highly infectious diseases safely and securely to regional treatment centers.

“Saving lives during crises requires preparation and training,” explained HHS Assistant Secretary for Preparedness and Response Robert Kadlec, M.D. “A tremendous amount of coordination, synchronization, and skill is needed to move patients with highly infectious diseases safely. We have to protect the patients and the healthcare workers caring for those patients. This type of exercise helps ensure that everyone involved is ready for that level of complexity.”
Coordinated by the HHS Office of the Assistant Secretary for Preparedness and Response, more than 50 organizations will participate, including the Department of State, Department of Transportation, the Regional Ebola Treatment Centers, local and state health and emergency management agencies, hospitals, airport authorities, and non-government organizations.
Throughout the exercise, participants react as if the incident is real. They must take the necessary actions and employ the appropriate resources to manage and protect the patients, the workforce and the environment and safely transport the patients.
The exercise focuses on moving seven people acting as patients with Ebola symptoms in different regions of the country. The patients, including one pediatric patient, first present themselves at one of the following healthcare facilities: CHI St. Luke’s Health-The Woodlands Hospital in The Woodlands, Texas; Medical University of South Carolina in Charleston, South Carolina; Norman Regional Hospital in Norman, Oklahoma; St. Alphonsus Regional Medical Center in Boise, Idaho, and St. Luke’s Regional Medical Center in Boise, Idaho.
At each facility, healthcare workers will collect and ship samples for diagnostic tests to state laboratories, which in turn will practice running the necessary laboratory tests to diagnose the patients with Ebola. As part of the exercise, each patient will receive a positive diagnosis. Using appropriate isolation techniques and personal protective equipment, health care workers then must take steps to have six of the patients transported by air to designated Regional Ebola Treatment Centers. These patients will be placed into mobile biocontainment units for these flights. The pediatric patient will be placed into protective equipment and transported by ground ambulance.
The treatment centers that will receive the patients are Cedars-Sinai Medical Center in Los Angeles, California; Emory University Hospital in Atlanta, Georgia; Providence Sacred Heart Medical Center in Spokane, Washington; and University of Texas Medical Branch in Galveston, Texas. The pediatric patient will be transported to Texas Children’s Hospital West Campus in Houston, Texas.
The participating airports are Boise Airport in Boise, Idaho; Charleston International Airport in Charleston, South Carolina; DeKalb-Peachtree Airport in Atlanta, Georgia; Ellington Field Airport in Houston, Texas; Los Angeles International Airport in Los Angeles, California; Spokane International Airport in Spokane, Washington; and Will Rogers World Airport in Oklahoma City, Oklahoma. Upon arrival, local emergency responders will transfer the patients to ground ambulances for transportation from the airports to the treatment centers.
HHS and the Department of State previously collaborated on exercises to move Americans acting as Ebola patients from West African countries to Ebola treatment centers in the United States. In public health emergencies or disasters, the U.S. government orchestrates the return of Americans to the United States, including Americans who are sick or injured.
This exercise runs through April 12. Participants will gather on April 13 to assess the exercise, compare actions across the country, and share best practices for moving patients with highly infectious diseases.
Note to editors: Video sound bites from Dr. Kadlec are available for download at https://www.dropbox.com/sh/ktvdv44y7z68ly7/AAAf2H_JzzY8i-tzREY6VfaAa?dl=0 ![]() .
.
