Hurricane Michael Advisory Number 15
NWS National Hurricane Center Miami FL AL142018
400 AM CDT Wed Oct 10 2018
…EXTREMELY DANGEROUS CATEGORY 4 MICHAEL STRENGTHENS
FURTHER AS IT HEADS NORTHWARD TOWARD THE FLORIDA PANHANDLE…
…LIFE-THREATENING STORM SURGE…HURRICANE FORCE WINDS…AND HEAVY
RAINFALL EXPECTED ALONG THE NORTHEASTERN GULF COAST…
SUMMARY OF 400 AM CDT…0900 UTC…INFORMATION
———————————————-
LOCATION…28.3N 86.5W
ABOUT 140 MI…225 KM SSW OF PANAMA CITY FLORIDA
ABOUT 130 MI…215 KM SW OF APALACHICOLA FLORIDA
MAXIMUM SUSTAINED WINDS…140 MPH…220 KM/H
PRESENT MOVEMENT…N OR 360 DEGREES AT 13 MPH…20 KM/H
MINIMUM CENTRAL PRESSURE…943 MB…27.85 INCHES
WATCHES AND WARNINGS
——————–
CHANGES WITH THIS ADVISORY:
A Tropical Storm Warning is now in effect from South Santee River,
South Carolina to Surf City, North Carolina.
The Storm Surge Watch has been discontinued west of the
Okaloosa/Walton County Line Florida.
SUMMARY OF WATCHES AND WARNINGS IN EFFECT:
A Storm Surge Warning is in effect for…
* Okaloosa/Walton County Line Florida to Anclote River Florida
A Storm Surge Watch is in effect for…
* Anclote River Florida to Anna Maria Island Florida, including
Tampa Bay
A Hurricane Warning is in effect for…
* Alabama/Florida border to Suwannee River Florida
A Tropical Storm Warning is in effect for…
* Alabama/Florida border to the Mississippi/Alabama border
* Suwanee River Florida to Chassahowitzka Florida
* North of Fernandina Beach Florida to Surf City North Carolina
A Tropical Storm Watch is in effect for…
* Chassahowitzka to Anna Maria Island Florida, including Tampa Bay
* Mississippi/Alabama border to the Mouth of the Pearl River
* Surf City North Carolina to Duck North Carolina
* Pamlico and Albemarle Sounds
A Storm Surge Warning means there is a danger of life-threatening
inundation, from rising water moving inland from the coastline,
during the next 36 hours in the indicated locations. For a depiction
of areas at risk, please see the National Weather Service Storm
Surge Watch/Warning Graphic, available at hurricanes.gov. This is
a life-threatening situation. Persons located within these areas
should take all necessary actions to protect life and property from
rising water and the potential for other dangerous conditions.
Promptly follow evacuation and other instructions from local
officials.
A Hurricane Warning means that hurricane conditions are expected
somewhere within the warning area, in this case within the next
12 hours. Preparations to protect life and property should be
rushed to completion.
A Tropical Storm Warning means that tropical storm conditions are
expected somewhere within the warning area, in this case during the
next 12 hours.
A Storm Surge Watch means there is a possibility of life-
threatening inundation, from rising water moving inland from the
coastline.
A Tropical Storm Watch means that tropical storm conditions are
possible within the watch area.
Interests elsewhere across the southeastern United States should
monitor the progress of Michael.
For storm information specific to your area, including possible
inland watches and warnings, please monitor products issued by your
local National Weather Service forecast office.
DISCUSSION AND OUTLOOK
———————-
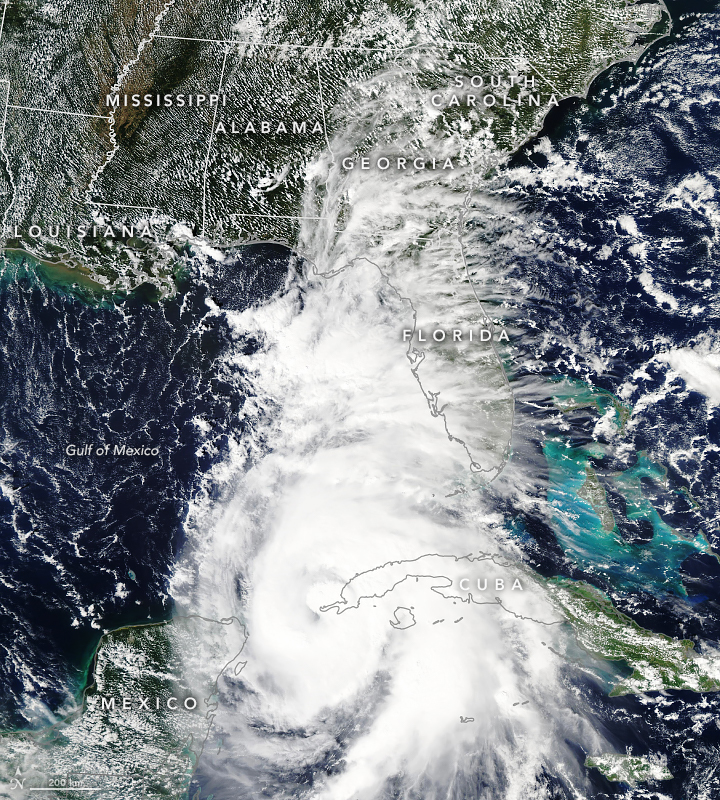
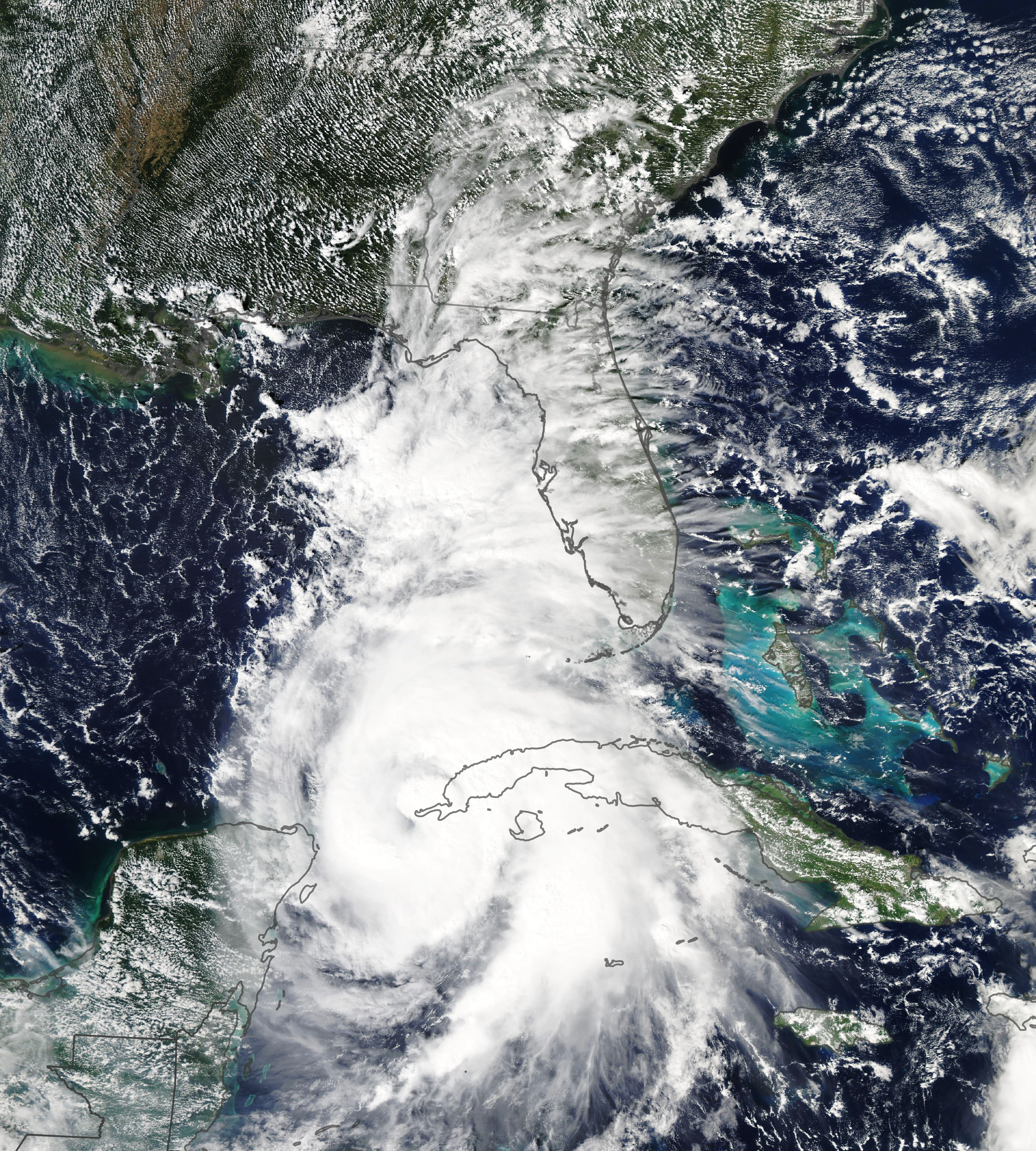
At 400 AM CDT (0900 UTC), the eye of Hurricane Michael was located
near latitude 28.3 North, longitude 86.5 West. Michael is moving
toward the north near 13 mph (20 km/h). A turn toward the north-
northeast is expected this morning, with a turn toward the northeast
expected this afternoon or tonight. A motion toward the northeast at
a faster forward speed is forecast on Thursday and Friday. On the
forecast track, the eye of Michael is expected to move ashore over
the Florida Panhandle later today, move northeastward across the
southeastern United States tonight and Thursday, and then move off
the Mid-Atlantic coast away from the United States on Friday.
Reports from an Air Force Reserve Hurricane Hunter aircraft indicate
that maximum sustained winds have increased to near 140 mph (220
km/h) with higher gusts. Michael is an extremely dangerous category
4 hurricane on the Saffir-Simpson Hurricane Wind Scale. Some
additional strengthening is possible before landfall. After
landfall, Michael should weaken as it crosses the southeastern
United States.
Hurricane-force winds extend outward up to 45 miles (75 km) from the
center and tropical-storm-force winds extend outward up to 185 miles
(295 km). NOAA buoy 42039 to the northeast of the center recently
reported sustained winds of 54 mph (85 km/h) and a wind gust of
63 mph (101 km/h).
The estimated minimum central pressure based on Hurricane Hunter
aircraft data is 943 mb (27.85 inches).
HAZARDS AFFECTING LAND
———————-
STORM SURGE: The combination of a dangerous storm surge and the
tide will cause normally dry areas near the coast to be flooded by
rising waters moving inland from the shoreline. The water has the
potential to reach the following heights above ground if peak surge
occurs at the time of high tide…
Tyndall Air Force Base FL to Keaton Beach FL…9-13 ft
Okaloosa/Walton County Line FL to Tyndall Air Force Base FL…6-9 ft
Keaton Beach FL to Cedar Key FL…6-9 ft
Cedar Key FL to Chassahowitzka FL…4-6 ft
Chassahowitzka to Anna Maria Island FL including Tampa Bay…2-4 ft
WIND: Hurricane conditions are expected within the hurricane
warning area along the U.S. Gulf Coast today, with tropical storm
conditions expected to begin during the next few hours. Hurricane
conditions will also spread well inland across portions of the
Florida Panhandle, southeastern Alabama and southwestern Georgia.
Tropical storm conditions are expected in the tropical storm warning
area during the next several hours, and are possible within the
tropical storm watch area by that time. Hurricane conditions are
possible within the hurricane watch area today.
Tropical storm conditions are expected to spread northward within
the warning area along the southeast U.S. coast beginning tonight,
and are possible in the watch area by late Thursday and Thursday
night.
RAINFALL: Michael is expected to produce the following rainfall
amounts through Friday…
Florida Panhandle and Big Bend, southeast Alabama, and portions of
southwest and central Georgia…4 to 8 inches, with isolated maximum
amounts of 12 inches. This rainfall could lead to life-threatening
flash floods.
The remainder of Georgia, the Carolinas, and southern Virginia…3
to 6 inches, with isolated maximum amounts of 8 inches. This
rainfall could lead to life-threatening flash floods.
Florida Peninsula, eastern Mid Atlantic, southern New England
coast…1-3 inches.
SURF: Swells generated by Michael are affecting the coasts of the
eastern and northern Gulf of Mexico, and will spread to portions of
the northwestern and western Gulf of Mexico coast during the next
day or so. These swells are likely to cause life-threatening surf
and rip current conditions. Please consult products from your local
weather office.
TORNADOES: A few tornadoes will be possible across parts of the
Florida Panhandle and the northern Florida Peninsula through this
afternoon. This risk will spread into parts of central and southern
Georgia and southern South Carolina this afternoon and tonight.
NEXT ADVISORY
————-
Hourly position estimates will begin at 500 AM CDT.
Next intermediate advisory at 700 AM CDT.
Next complete advisory at 1000 AM CDT.
$$
Forecaster Beven
![[Image of probabilities of 34-kt winds]](https://www.nhc.noaa.gov/storm_graphics/AT14/refresh/AL142018_wind_probs_34_F120+png/033350.png)
![[Image of initial wind radii]](https://www.nhc.noaa.gov/storm_graphics/AT14/refresh/AL142018_current_wind+png/033350_current_wind_sm.png)

![[Image of cumulative wind history]](https://www.nhc.noaa.gov/storm_graphics/AT14/refresh/AL142018_wind_history+png/033350_wind_history.png)
![[Image of WPC Flash Flooding/Excessive Rainfall Outlook]](https://www.nhc.noaa.gov/storm_graphics/AT14/refresh/AL1418WPCERO+gif/033350WPCERO_sm.gif)