
Archive for November, 2018
Volcanologists report that Campi Flegrei , in and around which 1.5 million inhabitants live, is at the start of an eruption cycle
Thursday, November 15th, 2018
The Campi Flegrei caldera cluster is the largest volcanic feature along the Bay of Naples, which is also home to the more famous Vesuvius. The Campi Flegrei, or “Fiery Fields,” is built from a series of overlapping volcanic features—calderas, domes, and cinder cones—that are historically active.
The Campi Flegrei calderas have produced two of the largest eruptions Europe has seen in the past 40,000 years. The Neopolitan Yellow Tuff (rock composed of fragments of material embedded within volcanic ash) was erupted roughly 12,800 years ago, with a total volume of at least 40 cubic kilometers (10 cubic miles). The Campanian Ignimbrite (rock made from the fused remnants of a pyroclastic flow) is about 32,800 years old and has a volume of at least 100 cubic kilometers (20 cubic miles).
Since the Neopolitan Yellow Tuff was formed, numerous small eruptions have occurred in the caldera complex, mostly less than half a cubic kilometer (0.1 cubic miles) in size. The most recent eruption occurred in 1538 at Monte Nuovo, a small cinder cone; that strombolian activity killed at least 32 people.
The most obvious manifestation of the magma under the surface at the Campi Flegrei is the La Solfatara, a region of intense hydrothermal activity. There has also been repeated cycles of uplift and subsidence near the city of Pozzouli, sometimes on the order of meters per decade, along with degassing within the Gulf of Pozzouli.
This natural-color image was acquired by the Advanced Land Imager (ALI) aboard the Earth Observing-1 (EO-1) satellite on July 9, 2012.
NASA Earth Observatory image by Jesse Allen and Robert Simmon, using EO-1 ALI data from the NASA EO-1 team. Caption by Erik Klemetti, Eruptions Blog/Denison University.
11/14/1985: 25,000 lives were lost after the eruption of the Nevado del Ruiz volcano in Colombia
Wednesday, November 14th, 2018“…..The worst scene of destruction was the city of Armero. The wave of mud, rock and ice was nearly 100 feet high as it barreled down on the city……”
8 new cases along with 4 more deaths from EBV: 3 health zones in the Democratic Republic of Congo (DRC) reported their first confirmed Ebola cases
Wednesday, November 14th, 2018

Increase in Acute Flaccid Myelitis — United States, 2018
Wednesday, November 14th, 2018McKay SL, Lee AD, Lopez AS, et al. Increase in Acute Flaccid Myelitis — United States, 2018. MMWR Morb Mortal Wkly Rep. ePub: 13 November 2018. DOI: http://dx.doi.org/10.15585/mmwr.mm6745e1.
n August 2018, CDC noted an increased number of reports of patients having symptoms clinically compatible with acute flaccid myelitis (AFM), a rare condition characterized by rapid onset of flaccid weakness in one or more limbs and spinal cord gray matter lesions, compared with August 2017. Since 2014, CDC has conducted surveillance for AFM using a standardized case definition (1,2). An Epi-X* notice was issued on August 23, 2018, to increase clinician awareness and provide guidance for case reporting.
Patients who meet the clinical case criteria for AFM, defined as acute flaccid limb weakness, are classified using the Council of State and Territorial Epidemiologists case definitions of “confirmed” (magnetic resonance imaging [MRI] with spinal cord lesion largely restricted to gray matter and spanning ≥1 spinal segments), “probable” (cerebrospinal fluid [CSF] pleocytosis [>5 white blood cells per mm3]), or “not a case.”
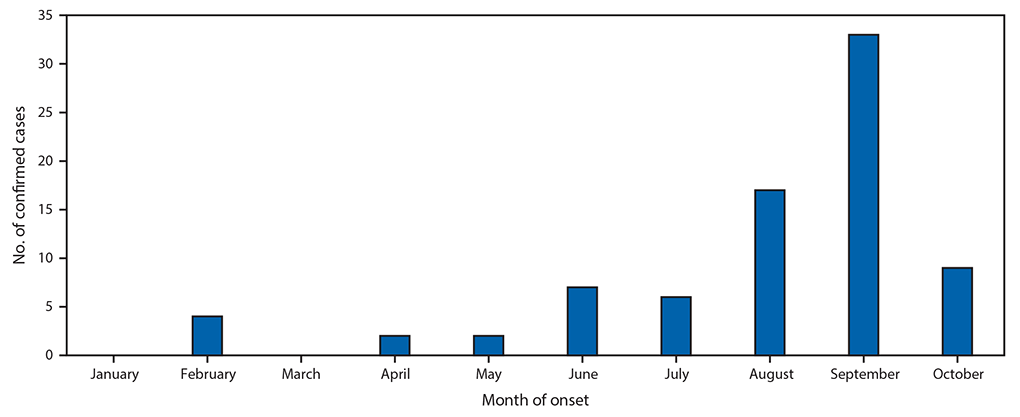
Among 106 patients with acute flaccid limb weakness classified during January 1–November 2, 2018, 80 cases of AFM were classified as confirmed (from 25 states) (Figure), 6 as probable, and 20 as noncases. This represents a threefold increase in confirmed cases compared with the same period in 2017. Among confirmed cases, the median patient age was 4 years (range = 7 months–32 years; interquartile range [IQR] = 2.4–7.6 years), 47 (59%) were male, and, among 65 patients with information on race available, 56 (86%) were white. During the 4 weeks preceding the onset of limb weakness, signs and symptoms consistent with a viral illness were reported for 79 (99%), including fever for 65 (81%), respiratory symptoms (e.g., cough, rhinorrhea, and congestion) for 62 (78%), and gastrointestinal symptoms (e.g., vomiting and diarrhea) for 30 (38%) patients with confirmed AFM. Upper limb only involvement was reported by 38 (47.5%) patients, lower limb only by 7 (8.8%), two to three upper and lower limbs by 12 (15.0%), and all four limbs by 23 (28.8%). All patients with confirmed AFM were hospitalized, and 47 (59%) were admitted to intensive care units; no deaths have been reported.
Among 78 (98%) confirmed cases with available CSF results, 65 (83%) had pleocytosis, with a median cell count of 103 cells per mm3 (range = 6–814; IQR = 56–194); most had a lymphocyte predominance. Median CSF protein and glucose were 47 mg per dL (range = 8–289; IQR = 37–62; normal <45) and 59 mg per dL (range = 40–138; IQR = 52–65; normal ≥40), respectively. The median interval from limb weakness to CSF collection was 1 day (range = 0–16; IQR = 1–3). The median interval from sign or symptom onset to CSF collection was 7 days (range = 0–23; IQR = 5–8) for respiratory illness, 4 days (range = 0–22; IQR = 3–7) for gastrointestinal symptoms, and 3 days (range = 0–17; IQR = 2–6) for fever.
CDC conducts enterovirus/rhinovirus (EV/RV) testing for all patients meeting the clinical criteria for AFM, when specimens are available. Of the 80 confirmed cases in 2018, testing was performed on a total of 125 clinical specimens from 71 (89%) patients, including 21 CSF, 59 upper respiratory, and 45 stool/rectal swab specimens (Table). Among these, specimens from 38 (54%) patients were positive by EV/RV real-time reverse transcription–polymerase chain reaction testing, including 11 (29%) for EV-A71, 14 (37%) for EV-D68, and 13 (34%) for other viruses, primarily from nonsterile sites. CSF specimens from two patients were positive. One CSF specimen was positive for EV-A71; this patient also had a stool specimen positive for EV-A71. The second patient had a CSF specimen positive for EV-D68; this patient also had EV-D68 and parechovirus-A6 identified in a respiratory specimen. Two additional patients had more than one virus detected in a single respiratory specimen, including one with EV-D68 and echovirus 6 and one with RV-A24 and parechovirus-A6. All stool specimens tested negative for poliovirus. Among the 20 patients who did not meet the AFM case definition and were classified as noncases, 1 (5%) had a positive CSF specimen (echovirus 25), 7 (35%) had positive respiratory specimens (EV-A71, RV-A24, RV-A56, RV-A90, EV/RV not typed), and 6 (30%) had positive stool or rectal swab specimens (EV-D68, EV-A71, RV-A90, echovirus 9, echovirus 11, echovirus 25).
Because some enteroviruses can cause acute flaccid limb weakness, and there was a temporal association with AFM and a nationwide severe respiratory outbreak of EV-D68 in 2014 (2), CDC performs EV/RV testing in an effort to identify etiologies for AFM cases. Despite a subsequent peak of AFM in 2016 (https://www.cdc.gov/acute-flaccid-myelitis/afm-surveillance.html), CDC did not receive reports of large outbreaks of severe respiratory illness in 2016. Further, there has been limited detection of pathogens in CSF in these cases; virus identified in CSF would be considered etiologic. Almost all patients with AFM have reported signs and symptoms consistent with viral illness in the weeks preceding limb weakness. Clinical, laboratory, and epidemiologic evidence to date suggest a viral association. CDC and collaborators continue to investigate risk factors for AFM and to study the causes and mechanisms of AFM.
Parents and caregivers are urged to seek immediate medical care for a child who develops sudden weakness of the arms or legs. In the evaluation of a child with acute flaccid limb weakness, clinicians are advised to inquire about recent fever with or without antecedent respiratory or gastrointestinal symptoms and to collect timely specimens for viral testing, including CSF, serum, respiratory, and stool specimens. Additional information for clinicians is available at https://www.cdc.gov/acute-flaccid-myelitis/hcp/index.html. Patients with acute flaccid limb weakness should be reported to their health departments as soon as possible regardless of laboratory or MRI findings.
11/13/1970: An immense tidal wave and storm surge caused by a powerful cyclone kills over 200,000 people in East Pakistan (Bangladesh)
Tuesday, November 13th, 2018Female genital mutilation/cutting rates have seen a “huge and significant decline” among African girls in the last 2 decades
Tuesday, November 13th, 2018“……Using data from 29 countries and going back to 1990, the report’s authors found that the biggest fall in cutting was in East Africa.
The prevalence rate there dropped from 71% of girls under 14 in 1995, to 8% in 2016……”
, et al
Democratic Republic of Congo: The current Ebola outbreak is the most severe in the country’s history with 319 confirmed and probable cases and at least 198 dead.
Tuesday, November 13th, 2018“…..efforts to contain the deadly outbreak have been thwarted by violence against health officials and civilians as militant groups battle for control in the affected region. The minister said two health workers were killed in one attack……”
42 deaths & 200 missing: Camp Fire becomes deadliest in California’s history
Tuesday, November 13th, 2018“…..The Camp Fire, which decimated Paradise, has already burned about 117,000 acres and is only about 30 percent contained.….”
FDA authorizes emergency use of first Ebola fingerstick test with portable reader
Tuesday, November 13th, 2018FDA authorizes emergency use of first Ebola fingerstick test with portable reader
For Immediate Release
November 9, 2018
Release
Today, the U.S. Food and Drug Administration announced that an emergency use authorization (EUA) has been issued for a rapid, single-use test for the detection of Ebola virus (Zaire ebolavirus). This is the second Ebola rapid antigen fingerstick test available under EUA, but the first that uses a portable battery-operated reader, which can help provide clear diagnostic results outside of laboratories and in areas where patients are likely to be treated.
The test, called the DPP Ebola Antigen System, is used with blood specimens, including capillary “fingerstick” whole blood, from individuals with signs and symptoms of Ebola virus disease (EVD) in addition to other risk factors, such as living in an area with large numbers of EVD cases and/or having contact with other individuals exhibiting signs and symptoms of EVD.
“The scourge of Ebola tragically demonstrates that we’re a global community when it comes to public health protection. Infectious disease doesn’t recognize nation states. Bacteria and viruses don’t respect territorial boundaries. It takes a sustained, robust and globally coordinated effort to protect our nation and the global community from various infectious disease threats. We’re all in this together. To that end, our FDA team of experts in drugs, vaccines and diagnostics continue to collaborate with our Federal, international and industry partners to employ our collective expertise, experiences from previous incidents, and resources to assist in the global response to the Ebola outbreak in the Democratic Republic of Congo,” said FDA Commissioner Scott Gottlieb, M.D. “This EUA is part of the agency’s ongoing efforts to help mitigate potential, future threats by making medical products that have the potential to prevent, diagnosis or treat available as quickly as possible. We’re committed to helping the people of the DRC effectively confront and end the current Ebola outbreak. By authorizing the first fingerstick test with a portable reader, we hope to better arm health care providers in the field to more quickly detect the virus in patients and improve patient outcomes.”
The FDA’s EUA authority allows the agency to authorize the use of an unapproved medical product, or the unapproved use of an approved medical product when, among other circumstances, there are no adequate, approved and available alternatives. When circumstances exist justifying authorization, the EUA becomes an important mechanism that allows broader access to medical products that have not been FDA cleared or approved and are instead only authorized for use for the duration of an emergency declaration. The FDA’s criteria for issuing an EUA for a diagnostic test includes making an assessment that it is reasonable to believe, based on the totality of evidence available to the agency, that the test may be effective and the known and potential benefits of using the test outweigh its known and potential risks.
In 2014, during the Ebola outbreak in West Africa, an emergency was declared by the Secretary of Health and Human Services. While that outbreak has ended, ongoing, smaller Ebola outbreaks have continued, and the emergency declaration is still in place. Recent outbreaks in remote areas with limited resources can benefit from rapid diagnostic tools, and the issuance of an EUA for the DPP Ebola Antigen System is an important step in addressing these outbreaks.
The DPP Ebola Antigen System provides rapid diagnostic results with tests that can be performed in locations where a healthcare provider does not have access to authorized Ebola virus nucleic acid tests (PCR testing), which are highly sensitive but can only be performed in certain laboratory settings that are adequately equipped. The DPP Ebola Antigen System has been authorized for use with capillary “fingerstick” whole blood, ethylenediaminetetraacetic acid (EDTA, an anticoagulant added to whole blood to prevent coagulation) venous whole blood and EDTA plasma. The DPP Ebola Antigen System should only be run in facilities, including treatment centers and public health clinics where patients are likely to be treated, and laboratories that are adequately equipped, trained and capable of such testing.
While today’s action will increase access to diagnostic tools for healthcare providers who may not have otherwise been equipped to perform tests, it is important to note that a negative result from the DPP Ebola Antigen System, especially in patients with signs and symptoms of EVD, should not be used as the sole basis for patient management decisions. The diagnosis of EVD must be made based on multiple factors such as, history, signs, symptoms, exposure likelihood and other laboratory evidence in addition to the detection of Ebola virus.
The FDA remains committed to using its authorities and resources to advance the development of countermeasures to address emerging threats and recently outlined its efforts to help address Ebola virus outbreaks. The FDA will continue to work with its federal partners and potential commercial product manufacturers in the most expedited manner to increase the availability of authorized diagnostic tests for Ebola virus disease for emergency use during this and any future outbreak.
With the issuance of the EUA for the DPP Ebola Antigen System to Chembio Diagnostic Systems Inc., the FDA has now issued EUAs for nine nucleic acid tests and two rapid diagnostic tests for Ebola virus detection in human specimens.
The FDA, an agency within the U.S. Department of Health and Human Services, protects the public health by assuring the safety, effectiveness, and security of human and veterinary drugs, vaccines and other biological products for human use, and medical devices. The agency also is responsible for the safety and security of our nation’s food supply, cosmetics, dietary supplements, products that give off electronic radiation, and for regulating tobacco products.
###