Archive for April, 2019
Indonesia lifted a tsunami warning but urged people to remain vigilant and evacuate to higher ground after an earthquake of magnitude 6.8 struck off the coast of its island of Sulawesi.
Friday, April 12th, 2019
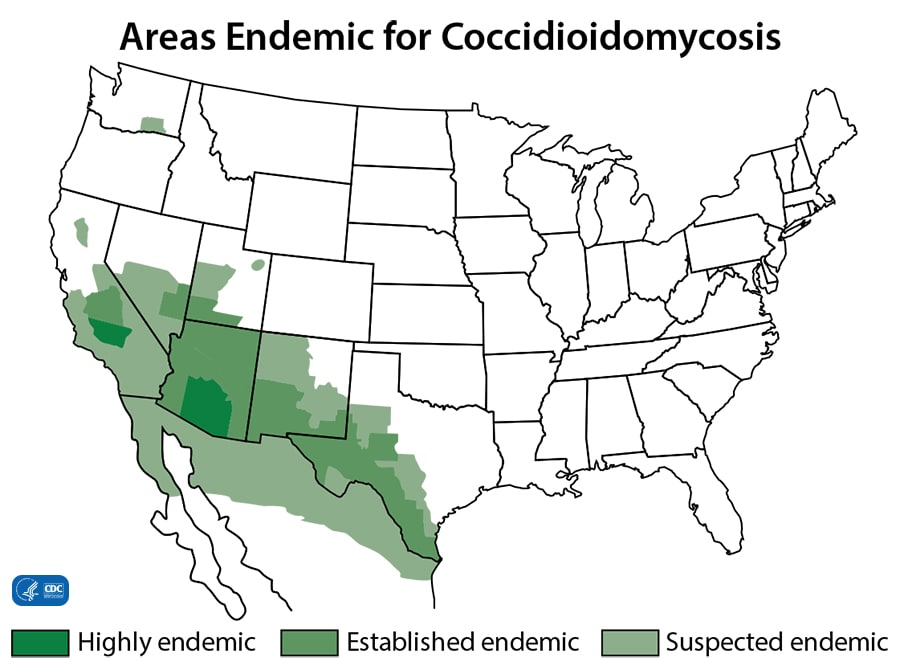
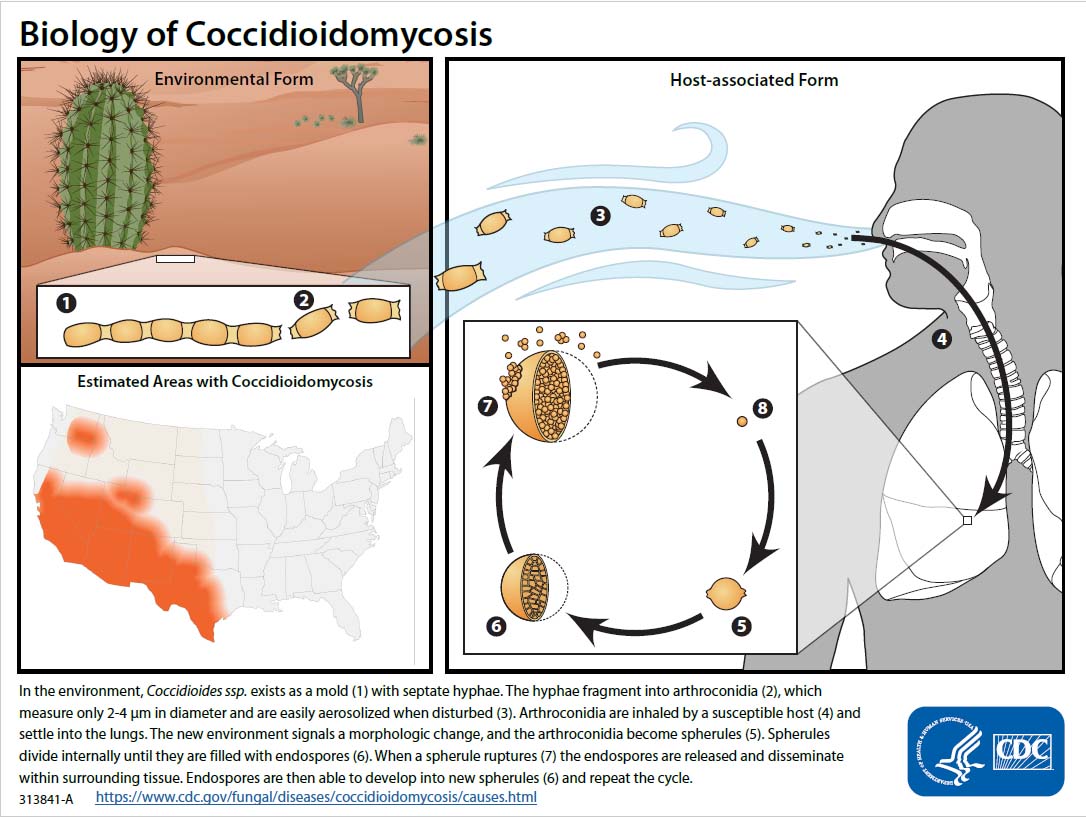
Returning from Community Service Trips to Baja California, Mexico: Coccidioidomycosis
Friday, April 12th, 2019Toda M, Gonzalez FJ, Fonseca-Ford M, et al. Notes from the Field: Multistate Coccidioidomycosis Outbreak in U.S. Residents Returning from Community Service Trips to Baja California, Mexico — July–August 2018. MMWR Morb Mortal Wkly Rep 2019;68:332–333. DOI: http://dx.doi.org/10.15585/mmwr.mm6814a5External.
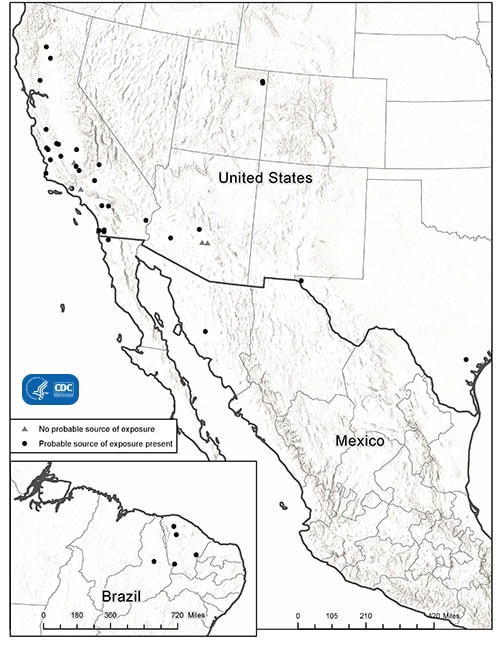
Cases of coccidioidomycosis among U.S. residents returning from community service trips to Baja California, Mexico (N = 8), by date of travel and date of illness onset — Kansas, Maryland, Michigan, and New York, July–August, 2018
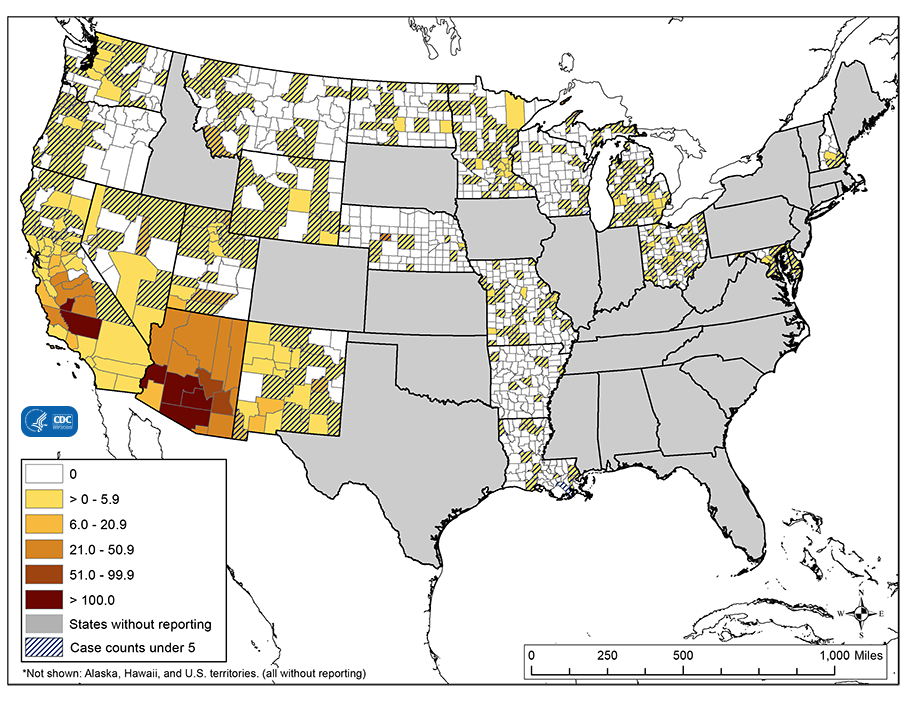
This map shows the average incidence of reported Valley fever per 100,000 people, by county, during 2010–2015. The rates in counties with fewer than five reported Valley fever cases, indicated by cross-hatching, might not be reliable. On this map, cases of Valley fever are classified according to people’s county of residence, which may not be where they acquired the infection. Cases in areas outside of regions where the fungus Coccidioides is believed to live are likely associated with travel to those disease-endemic areas.
FBI: Active Shooter Incidents in the United States in 2018
Friday, April 12th, 2019By the Numbers
* 27 incidents in 16 states
* 213 casualties – excluding the shooters
* 85 killed
* 2 law enforcement officers killed
* 1 unarmed security officer
* 128 wounded
* 6 law enforcement officers wounded
* 27 shooters – 23 male, 3 female, 1 at large
* 10 committed suicide
* 11 apprehended by police
* 4 killed by police
* 1 killed by citizens
* 1 at large
* 9 incidents ended with the exchange of gunfire between the shooters and law enforcement
The 27 active shooter incidents occurred in 16 states.
■ Four incidents occurred in California.
■ Three incidents occurred in Florida.
■ Two incidents occurred in each of the following states: Illinois, Kentucky, Maryland, New Mexico, Pennsylvania,
and Texas.
■ One incident occurred in each of the following states: Alabama, Georgia, Indiana, Ohio, Oklahoma, Tennessee,
Washington, and Wisconsin.
Ten of the 27 incidents met the criteria cited in the federal definition of “mass killings,” that is, “three or more
killings in a single incident.
Mozambique: A successful six-day emergency cholera vaccination campaign that reached more than 800 000 people
Thursday, April 11th, 2019WHO
10 April 2019, Maputo – The Ministry of Health in Mozambique has concluded a successful six-day emergency cholera vaccination campaign that reached more than 800 000 people in four districts affected by Cyclone Idai.
The campaign was supported by around 1200 community volunteers and partners including the World Health Organization (WHO), UNICEF, Médecins Sans Frontières (MSF), International Federation of the Red Cross and Red Crescent Societies (IFRC) and Save the Children.
“From start to finish, this campaign was one of the fastest ever, thanks to experienced people at the Ministry of Health, who knew there was a high risk of a cholera outbreak and made a rapid request for the vaccines as soon as the cyclone hit,” says Dr Djamila Cabral, Head of the WHO office in Mozambique. “The Ministry did an excellent job organizing the campaign and reaching so many people in such a short time. The oral cholera vaccine is one of the vital measures that can help save lives and stop the spread of this terrible disease during an outbreak.”
The oral cholera vaccines, donated by Gavi from the Global Cholera Vaccine Stockpile, arrived in Beira on Tuesday 2 April and, within 24 hours, began reaching people in need.
The vaccines were given to communities identified by the Government at highest risk – those without access to safe water and sanitation – in Beira, Dondo, Nhamatanda and Buzi districts.
Vaccine uptake has been very high and the campaign has been well received by the communities. Remaining vaccines will be used for other at-risk communities that were not reached by the initial campaign.
People develop protection against cholera approximately 7 days after receiving the vaccine. One dose of this oral vaccine provides around 85% protection against cholera for 6 months.
“Controlling cholera in these areas will reduce the risk to the rest of the population because fewer people will be taking it back and forth into the wider community,” says WHO cholera vaccination expert, Kate Alberti, who was deployed to Beira to support the Ministry of Health to organize the campaign.
Dr Nazira Abdula, Minister of Health of Mozambique, acknowledged the great support of WHO and partners for the vaccination campaign. “It’s very difficult to roll out a campaign of this scope in only three days,” she says.
WHO’s Dr Cabral adds: “This campaign would not have been possible without the strong engagement of the local authorities and the communities themselves. The number of volunteers is impressive and, wherever they go, there has been very strong uptake of the vaccine. Everyone is very keen to make this a success to stop cholera in its tracks.”
Since Cyclone Idai struck Mozambique on 14 March, hundreds of thousands of people have been living in temporary settlements without access to safe water and sanitation. The Ministry of Health declared a cholera outbreak on 27 March and, as of 8 April, had reported more than 3577 cases and 6 deaths.
The cholera vaccine is just one tool for the outbreak response. Currently 12 cholera treatment centres, with 500-bed capacity, have been set up by the national authorities and international partners to serve the affected communities. Partners are also supporting the local authorities to provide access to safe water and sanitation in settlements and communities across Sofala Province.
Cholera is endemic in several parts of Sofala province and the cholera outbreak that developed post-Cyclone Idai acts as a reminder that sustainable access to safe water, sanitation, and hygiene (WASH) is the long-term solution to controlling cholera. Acknowledging that every case of cholera is preventable, the Global Task Force on Cholera Control is implementing a Cholera Global Roadmap to 2030, which calls upon development partners and donors to support countries to reduce cholera deaths by 90% by 2030.
The recent escalation in the number of Ebola virus disease (EVD) cases continues in the Democratic Republic of the Congo
Thursday, April 11th, 2019April 9
“….This past week saw 65 new confirmed cases reported in the last seven days….”
“……Knowledge gained following the 2014–16 West Africa Ebola outbreak identified a number of challenges survivors face, including reduced or blurred vision stemming from inflammation of their eyes…..Next steps will be to continue to follow up with survivors, at the clinics held each month, where they are provided medical, biological and psychological care. There are currently over 300 survivors registered in the follow-up programme……”


Durham, North Carolina: One person has been killed and at least 15 are injured after an explosion and massive fire consumes a building downtown
Wednesday, April 10th, 2019Several African countries are still reporting monkeypox cases in 2019
Wednesday, April 10th, 2019Central African Republic: 34 cases have been reported, including two deaths.
Republic of Congo: Nine total cases have been reported with no fatalities.
Democratic Republic of the Congo: 824 total cases have been reported, including 12 deaths.
Nigeria: 311 cases (132 confirmed) and seven fatalities have been recorded.
Ready or Not: Protecting the Public’s Health from Diseases, Disasters and Bioterrorism, 2019
Tuesday, April 9th, 2019“One lesson from recent events is that emergencies happen. And happen often. From disease outbreaks to natural disasters to man-made crises, the stakes are high: Americans face serious health risks and even death with increasing regularity. Therefore, as a nation, it’s critical to ask, “Are we prepared?”
Executive Summary
The public health emergencies of the past year—an unusually severe flu season, confounding cases of acute flaccid myelitis, two major hurricanes, and the deadliest fire season in California’s history reinforce the need for every jurisdiction to be vigilant about preparing for emergencies in order to safeguard the public’s health.
A fundamental role of the public health community is to protect communities from disasters and disease outbreaks. To this end, the nation’s health security infrastructure has made tremendous strides since 2001 by building modern laboratories, maintaining a pipeline of medical countermeasures, and recruiting and retaining a workforce trained in emergency operations. Yet, unstable and insufficient funding puts this progress at risk, and a familiar pattern takes shape: underfunding, followed by a disaster or outbreak, then an infusion of onetime supplemental funds, and finally a retrenchment of money once attention wanes. What’s more, states are uneven in their levels of preparedness. Some—often those that most frequently face emergencies—have the personnel, systems, and resources needed to protect the public. But others are less prepared and less experienced, elevating the likelihood of preventable harms. This unstable funding and uneven preparation undermines America’s health security.
The Ready or Not: Protecting the Public’s Health from Diseases, Disasters and Bioterrorism series, produced by Trust for America’s Health (TFAH), has tracked public health emergency preparedness in the United States since 2003. The series has documented significant progress in the nation’s level of preparedness as well as those areas still in need of improvement.
Ready or Not examines the country’s level of public health emergency preparedness on a state-by-state basis using 10 priority indicators. (See Table 1.) Taken together, the indicators are a checklist of priority aspects of states’ readiness for public health emergencies. However, these indicators do not necessarily reflect the effectiveness of states’ public health departments. Improvement in these priority areas often requires action from other agencies, elected officials or the private sector.
The 2019 report finds that states have made progress in key areas, including public health funding and participation in provider compacts and coalitions. However, performance in other areas—such as flu vaccination, hospital patient safety, and paid time off for workers—has stalled or lost ground.
Table 1: Top-Priority Indicators of State Public Health Preparedness
| Indicators | |||
| 1 | Incident Management: Adoption of the Nurse Licensure Compact. | 6 | Water Security: Percentage of the population who used a community water system that failed to meet all applicable health-based standards. |
| 2 | Cross-Sector Community Collaboration: Percentage of hospitals participating in healthcare coalitions. | 7 | Workforce Resiliency and Infection Control: Percentage of employed population with paid time off. |
| 3 | Institutional Quality: Accreditation by the Public Health Accreditation Board. | 8 | Countermeasure Utilization: Percentage of people ages 6 months or older who received a seasonal flu vaccination. |
| 4 | Institutional Quality: Accreditation by the Emergency Management Accreditation Program. | 9 | Patient Safety: Percentage of hospitals with a top-quality ranking (Grade A) on the Leapfrog Hospital Safety Grade. |
| 5 | Institutional Quality: Size of the state public health budget, compared with the past year. | 10 | Health Security Surveillance: The public health laboratory has a plan for a six- to eight-week surge in testing capacity. |
Notes: The National Council of State Boards of Nursing organizes the Nurse Licensure Compact. The federal Hospital Preparedness Program of the U.S. Office of the Assistant Secretary for Preparedness and Response supports healthcare coalitions. The U.S. Environmental Protection Agency assesses community water systems. Paid time off includes sick leave, vacation time, or holidays, among other types of leave. The Leapfrog Group is an independent nonprofit organization. Every indicator, and some categorical descriptions, were drawn from the NHSPI, with one exception: public health funding. See “Appendix A: Methodology” for a description of TFAH’s funding data-collection process, including its definition.
Source: National Health Security Preparedness Index.
For the first time, Ready or Not groups states and the District of Columbia into one of three tiers based on their performance across the 10 indicators. This year, 17 states scored in the top tier, 20 and the District of Columbia placed in the middle tier, and 13 were in the bottom tier. (See Table 2).
By gathering together timely data on all 50 states and the District of Columbia, the report assists states in benchmarking their performance against comparable jurisdictions. To help states track their own progress, TFAH will strive to maintain continuity among the indicators tracked in this edition of the report for the next several years.
Table 2: State Public Health Emergency Preparedness
State performance, by scoring tier, 2018
| Performance Tier | States | Number of States |
| Top Tier | AL, CO, CT, FL, ID, KS, MA, MD, MO, MS, NC, NE, NJ, RI, VA, WA, WI | 17 states |
| Middle Tier | CA, DC, GA, HI, IA, IL, LA, ME, MI, MN, MT, ND, NH, NM, NV, OK, OR, SC, TX, VT, WV | 20 states and DC |
| Bottom Tier | AK, AR, AZ, DE, IN, KY, NY, OH, PA, SD, TN, UT, WY | 13 states |
Report Findings
A majority of states have made preparations to expand capabilities in an emergency, often through collaboration. In 2018, 31 states participated in the Nurse Licensure Compact, which allows registered nurses and licensed practical or vocational nurses to practice in multiple jurisdictions with a single license. In an emergency, this enables health officials to quickly increase their staffing levels. For example, nurses may cross state lines to lend their support at evacuation sites or other healthcare facilities. The number of states participating in the compact is up by five from 26 in 2017.
In addition, hospitals in most states have a high degree of participation in healthcare coalitions. On average, 89 percent of hospitals were in a coalition and 18 states had universal coalition participation, meaning every hospital in the state was part of a coalition. Such coalitions bring hospitals and other healthcare facilities together with emergency management and public health officials to plan for, and respond to, events requiring extraordinary action. This increases the likelihood that patients are served in a coordinated and efficient manner during an emergency.
Finally, 44 states and the District of Columbia had a plan to surge public health laboratory capacity for six to eight weeks as necessary during overlapping emergencies or large outbreaks.
Most residents who got their household water through a community water system had access to safe water. On average, just 6 percent of state residents used a community water system in 2017 that did not meet all applicable health-based standards. Water systems with such violations increase the chances of water-based emergencies in which contaminated water supplies place the public at risk.
Most states are accredited in the areas of public health, emergency management, or both. In 2018, the Public Health Accreditation Board or the Emergency Management Accreditation Program accredited 42 states and the District of Columbia; 26 states were accredited by both groups. Eight states (Alaska, Hawaii, Indiana, New Hampshire, South Dakota, Texas, West Virginia, and Wyoming) were accredited by neither. Both programs help ensure that necessary emergency prevention and response systems are in place and staffed by qualified personnel.
Seasonal flu vaccination rate, already too low, fell further. The seasonal flu vaccination rate among Americans ages 6 months or older dropped from 47 percent in the 2016–2017 season to 42 percent in the 2017–2018 season. This drop-in coverage may have exacerbated the severity of the 2017-2018 influenza season and the high number of illnesses, hospitalizations and deaths due to flu. Healthy People 2020, a set of federal 10-year objectives and benchmarks for improving the health of all Americans by 2020, set a seasonal influenza vaccination-rate target of 70 percent annually.
In 2018, only 55 percent of employed state residents, on average, had access to paid time off. Those without such leave are more likely to work when they are sick and risk spreading infection. In the past, some infectious disease outbreaks have been linked to or exacerbated by the absence of paid sick leave.
Only 28 percent of hospitals, on average, earned a top-quality patient safety grade. Hospital safety scores measure performance on such issues as healthcare-associated infection rates, intensive-care capacity, nursing staff volume, and an overall culture of error prevention. In the absence of diligent actions to protect patient safety, deadly infectious diseases can take hold or strengthen.
Climate Change Increases Likelihood of Extreme Weather
According to the Center for Climate and Energy Solutions, a nonprofit advocacy group, climate change is expected to increase the frequency, intensity, and consequences of some types of extreme weather events, including:
- Drought, which can contribute to food insecurity and exacerbate wildfires.
- Extreme heat, which in a typical year already kills more people in the United States than hurricanes, lightning, tornadoes, earthquakes, and floods combined. Extreme heat is especially dangerous for medically vulnerable people. It also worsens droughts and increases the risk of wildfires.
- Heavy rains, which cause catastrophic flooding, landslides, and contaminated waterways.
- Hurricanes, which sometimes have more destructive wind speeds, precipitation, and storm surges.
- Wildfires, which can now burn more land and are more difficult to extinguish.
In 2017 alone, at least 15 extreme weather events across the globe were made more likely by climate change, according to studies published by the American Meteorological Society.
On top of possible federal action, states and localities can act to mitigate these threats, particularly the dangers they pose to people with health ailments or in poor living conditions. For example, land-use planning can reduce loss of life and property from wildfires. Zoning rules that limit building in flood-prone areas reduces the dangers from floods, and replacing nonpermeable surfaces with “green infrastructure,” such as rain gardens and bioswales, reduces stormwater runoff and subsequent flooding. In drought-prone areas, green infrastructure can retain stormwater for later use. Cooling centers can keep vulnerable populations safe during heat waves, and green roofs can reduce the urban heat island effect. Finally, preserving coastal wetlands, dunes, and reefs can help absorb storm surges from hurricanes.
Report Recommendations
There are a host of concrete actions to further protect the public’s health that TFAH recommends be taken by federal, state, and local officials; the healthcare system; academia; and the private or nongovernmental sectors.
Those that are of highest priority include:
- Providing stable, dedicated, and sufficient funding for preparedness activities and a significant funding increase for core public health capabilities.
- Establishing a complementary emergency response fund to accelerate crisis responses.
- Maintaining a long-term investment in the Global Health Security Agenda framework and global preparedness and response programs to help prevent infectious disease threats from becoming global crises.
- Fully implementing the National Biodefense Strategy including with transparent goals, implementation plans, and budgets for all relevant agencies.
- Monitoring and addressing any potential challenges caused by the transition of the Strategic National Stockpile and significantly strengthening the “last mile” of distribution and dispensing.
- Developing a multiyear strategic vision, and fully funding surveillance infrastructure, for fast, accurate outbreak detection at all levels of government.
- Bolstering the Hospital Preparedness Program and multisector healthcare collaboration as well as adopting state policies to improve healthcare delivery during disasters.
- Adopting comprehensive climate change adaptation plans, including a public health assessment and response.
- Increasing public and private investments in efforts to combat antimicrobial resistance, including through diagnostic, stewardship, detection, and treatment methods.
- Supporting vaccine infrastructure and first-dollar coverage of recommended vaccines.
- Promoting health equity in emergency preparedness planning, response, and recovery, including through the appointment of a chief equity or resilience officer.
Taken together, action on TFAH’s recommendations would make the United States safer for all its residents.
CDC: Personal provisions, supplies, and equipment necessary to protect the health and safety of your family in an emergency.
Tuesday, April 9th, 2019The Basics
- Water
- Store at least 1 gallon of water per day for each person and each pet. You should consider storing more water than this for hot climates, for pregnant women, and for persons who are sick.
- Store at least a 3-day supply of water for each person and each pet. Try to store a 2-week supply, if possible.
- Observe the expiration date for store-bought water. Replace non-store bought water every 6 months.
- Store a bottle of unscented liquid household chlorine bleach (label should say it contains between 5-6% and 8.25% of sodium hypochlorite) to disinfect your water, if necessary, and to use for general cleaning and sanitizing.
- Nonperishable and ready-to-eat food, including special foods—such as nutrition drinks and ready-to-feed formula—for infants, people with dietary restrictions, food sensitivities and allergies, and medical conditions such as diabetes.
- Prescription eyeglasses, contact lenses, and contact lens solution.
- Assistive technologies, such as hearing aids and picture boards.
- Medical alert identification bracelet or necklace
- Health protection supplies, including insect repellentExternal, water purification tablets, and sunscreen.
- A change of clothes
- Medical equipment including:
- Canes, crutches, walkers, and wheelchairs
- Nebulizers
- Oxygen equipment
- Blood sugar monitors
- Medical supplies, including:
- Antibacterial wipes
- Catheters
- Syringes
- Nasal cannulas
- Blood test strips
- First aid supplies, including:
- First aid reference
- Non-latex gloves
- Digital thermometer
- Waterproof bandages and gauze
- Tweezers and scissors
- A Stop the Bleed kit, including a tourniquet
- Sanitation and hygiene items, including:
- Soap
- Hand sanitizer
- Sanitizing wipes
- Garbage bags and plastic ties
- Toilet paper
- Feminine hygiene supplies
- Pet supplies
- Childcare supplies
- Baby supplies