Archive for the ‘Bioterrorism’ Category
Synthetic Bioterrorism: New genetic tools are making it easier and cheaper to engineer viruses and bacteria in the lab and potentially making them more contagious and lethal.
Sunday, July 29th, 2018Biodefense in the Age of Synthetic Biology: http://nap.edu/24890
ISBN 978-0-309-46518-2 | DOI 10.17226/24890
Committee on Strategies for Identifying and Addressing Potential Biodefense
Vulnerabilities Posed by Synthetic Biology; Board on Chemical Sciences and
Technology; Board on Life Sciences; Division on Earth and Life Studies;
National Academies of Sciences, Engineering, and Medicine
One danger is making existing bacteria or viruses more dangerous by giving them antibiotic resistance or altering them so that they produce toxins or evade vaccines.
“…..in a table-top exercise conducted last month by the Johns Hopkins Center for Health Security…..experts in pandemic response and national security grappled with a fictional virus called “Clade X” that was created by a terrorist group that inserted genetic elements of deadly Nipah virus into a normally-mild human parainfluenza virus.
The terrorist group in this scenario wanted to depopulate the Earth, and deliberately released the contagious virus at multiple spots around the globe. The resulting pandemic killed 150 million people within a year as officials struggled to contain the social and economic chaos until a vaccine could be made…….”
The tricky tularemia bacterium
Thursday, May 31st, 2018NIH scientists show how tularemia bacteria trick cells to cause disease
 A female Aedes mosquito.NIAID
A female Aedes mosquito.NIAIDWhat
Francisella tularensis is the bacterium that causes tularemia, a life-threatening disease spread to humans via contact with an infected animal or through mosquito, tick or deer fly bites. As few as 10 viable bacteria can cause the disease, which has a death rate of up to 60 percent. Scientists from the National Institute of Allergy and Infectious Diseases — part of the National Institutes of Health — have unraveled the process by which the bacteria cause disease. They found that F. tularensis tricks host cell mitochondria, which produce energy for the cell, in two different phases of infection. In the first eight hours of infection, the bacteria increase mitochondria function, which inhibits cell death and prevents the cell from mounting an inflammatory response to avoid an immune system attack. In the 24 hours after, the bacteria impair mitochondrial function, undergo explosive replication and spread. These basic science findings could play a role in developing effective treatment strategies, according to the researchers.
Previously, researchers discovered that F. tularensis could inhibit inflammation following infection of immune system cells called macrophages, but they did not understand how it occurred. The new study, published in Infection and Immunity, illuminates that process, confirming that the bacterium’s manipulation of the mitochondrial machinery in the host cell is required to block strong inflammatory responses. Also, the researchers show that the timing of the manipulation of the mitochondria machinery during infection is important to how the bacteria control host cell death. The researchers also said this could be the first study to show that a bacterium’s sugar-like protective outer capsule, or polysaccharide, can increase mitochondria function, in this case, during early infection.
The researchers believe that better antimicrobial treatment strategies — against F. tularensis and possibly other pathogens — could result from further study of the role the capsule polysaccharide plays in manipulating mitochondria. For example, learning how to block the increased mitochondrial function in phase one could limit infection, they say. In their study, they also treated F. tularensis-infected macrophages in the laboratory with two types of drugs that protect mitochondria. The treatment reduced cell death and limited bacterial replication. The group plans to extend that work to mice.
Article
F Jessop et al. Temporal manipulation of mitochondrial function by virulent Francisella tularensis to limit inflammation and control cell death. Infection and Immunity DOI: 10.1128/IAI.00044-18 (2018).
FDA issues final guidance for drug companies to use for developing pre-exposure prophylaxis for inhalational anthrax.
Friday, May 25th, 2018FDA In Brief: As part of a longstanding program encouraging the development of medical countermeasures; new FDA policy promotes innovation to thwart inhalational anthrax
May 23, 2018
Media Inquiries
Tara Rabin
240-402-3157
“The FDA has long played an important role preparing our nation for potential bioterrorism threats, providing guidance and support around the development of medical countermeasures that can be used safely, effectively and reliably during public health emergencies,” said FDA Commissioner Scott Gottlieb, M.D. “Since the 2001 anthrax attacks, the U.S. government’s efforts to protect the nation from bioterrorism threats have continued to evolve. We now know that a comprehensive preparedness plan for potential anthrax threats must account for both pre- and post-exposure scenarios. That’s why the FDA has taken steps to modernize its guidance on inhalational anthrax to advance the development of new drugs for prophylaxis, prior to exposure. This builds upon the treatments that are currently available for inhalational anthrax and advances the agency’s longstanding commitment to the development of a full suite of medical countermeasures as part of its established programs.”
The U.S. Food and Drug Administration today issued final guidance, Anthrax: Developing Drugs for Prophylaxis of Inhalational Anthrax, which is designed to assist in the development of drugs for prophylaxis (prevention) of inhalational anthrax for individuals who may be potentially exposed to or have inhaled aerosolized Bacillus anthracis (B. anthracis) spores, but who have not yet displayed related signs and symptoms.
While there are FDA-approved drugs for treatment of anthrax and for post-exposure prophylaxis of inhalational anthrax, situations can arise where starting therapy immediately before the anticipated or potential exposure can reduce the risk of illness and death (for example, first responders who anticipate an imminent risk of exposure to B. anthracis spores).
The FDA’s final guidance is the result of a multi-year effort to advance its policy framework for the development of treatments targeting inhalational anthrax. The final guidance revises the indication to “prophylaxis of inhalational anthrax” for the reduction of disease risk in those who have inhaled, or are likely to inhale, aerosolized B. anthracis spores, but who do not yet have established disease.
Clinical trials in humans cannot be conducted since naturally occurring inhalational anthrax is extremely rare and it would be unethical to deliberately expose healthy human volunteers to B. anthracis spores. Therefore, the final guidance clarifies that drugs developed for the prophylaxis of inhalational anthrax can rely on evidence from animal studies (known as the Animal Rule) to support approval when the criteria under the Animal Rule have been met.
The FDA encourages drug developers to reference the final guidance issued today when designing studies to appropriately establish the safety and effectiveness of drugs for prophylaxis of inhalational anthrax.
Related Information
The FDA, an agency within the U.S. Department of Health and Human Services, protects the public health by assuring the safety, effectiveness, and security of human and veterinary drugs, vaccines and other biological products for human use, and medical devices. The agency also is responsible for the safety and security of our nation’s food supply, cosmetics, dietary supplements, products that give off electronic radiation, and for regulating tobacco products.
US experts sound off: The USA ‘….is “woefully unprepared for these biological threats” in an increasingly interdependent world……’
Monday, April 30th, 2018- James Lawler is “…a retired Navy commander whose experience includes serving as director for medical preparedness policy on the National Security Council and director for biodefense policy on the White House’s Homeland Security Council…”
- “….Kenneth Luongo, president and founder of the Partnership for Global Security, echoed that the U.S. “remains woefully underprepared” for a biological attack or a “new intensity level” of pathogens…..”
- “….Former USAID Director Andrew Natsios, director of the Scowcroft Institute of International Affairs, told the panel that the country is “a lot more fragile than we realize” when it comes to emergency response….”
PHEMCE High-Priority Threats
Tuesday, January 2nd, 2018PHEMCE High-Priority Threats
The PHEMCE will continue to address MCM needs to protect against high-priority threats for which the Secretary of Homeland Security made a determination pose a material threat sufficient to affect national security or PHEMCE leadership determines to have the potential to threaten national health security.
This year, the PHEMCE added three chemical agents (chlorine, phosgene, and vesicants); otherwise, the high-priority threats are unchanged from those listed in the 2016 PHEMCE SIP. The PHEMCE high-priority threats are (in alphabetical order by threat area):
Biological Threats
- Bacillus anthracis (anthrax)* and
- Multi-drug resistant B. anthracis (MDR anthrax)*
- Burkholderia mallei (glanders)* and
- Burkholderia pseudomallei (melioidosis)*
- Clostridium botulinum toxin (botulism)*
- Ebola virus (Ebola hemorrhagic fever)*
- Emerging infectious diseases4
- Francisella tularensis (tularemia)*
- Marburg virus (Marburg hemorrhagic fever)*
- Pandemic influenza
- Rickettsia prowazekii (typhus)*
- Variola virus (smallpox)*
- Yersinia pestis (plague)*
- Chemical Threats
- Acetylcholinesterase inhibitor nerve agents*
- Chlorine5
- Cyanide salts (potassium and sodium cyanide)*
- Hydrogen cyanide*
- Phosgene5
- Vesicants*
- Radiological* and Nuclear* Threats(*) indicates threats identified under the following authorities related to MCMs: (1) emergency use authorities that rely on section 564(b)(1)(D) of the Federal Food, Drug, and Cosmetic Act (FD&C Act); (2) priority review vouchers PRVs) under section 565A of the FD&C Act;6 and, (3) procurements of security countermeasures under section 319F-2 of the PHS Act.
4 EIDs continue to remain a high-priority threat for the PHEMCE. The PHEMCE developed a risk assessment framework to assess whether specific emerging pathogens should be included explicitly as a high-priority threat. These pathogens may be included if PHEMCE leadership determines they have the potential to affect national health security.
5 The PHEMCE added additional chemical threat agents to the high-priority threat list after considering multiple factors, including recent reported intentional use of agents as weapons, accidental releases, availability of agents in industry, and health impacts of exposure.
6 It is possible that a drug product meeting the requirements of section 565A (material threat MCM priority review vouchers (PRVs)) also may meet the requirements of section 524 of the FD&C Act (which enables sponsors of certain tropical disease applications to receive PRVs). However, under section 565A(e), the same application is not permitted to receive more than one voucher. U.S. Food & Drug Administration (2017). Tropical Disease Priority Review Voucher Program. https://www.fda.gov/aboutfda/centersoffices/officeofmedicalproductsandtobacco/cder/ucm534162.htm and U.S. Food & Drug Administration (2017). 21st Century Cures Act: MCM-Related Cures Provisions. https://www.fda.gov/EmergencyPreparedness/Counterterrorism/MedicalCountermeasures/MCMLegalRegulatoryand PolicyFramework/ucm566498.htm#prv.
What is the PHEMCE?
Friday, December 29th, 2017The PHEMCE is an interagency coordinating body led by the HHS Assistant Secretary for Preparedness and Response, comprising the Centers for Disease Control and Prevention, the National Institutes of Health, the Food and Drug Administration, and interagency partners at the Departments of Defense, Veterans Affairs, Homeland Security, and Agriculture. It coordinates the development, acquisition, stockpiling, and recommendations for use of medical products that we need to effectively respond to a variety of high consequence public health emergencies, whether naturally occurring or intentional.
EXECUTIVE SUMMARY
The 2017-2018 Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) Strategy and Implementation Plan (SIP) describes the priorities that the U.S. Department of Health and Human Services (HHS), in collaboration with its interagency partners, will implement over the next five years. This strategy updates the 2016 PHEMCE SIP and fulfills the annual requirement established by Section 2811(d) of the Public Health Service (PHS) Act, as amended by the Pandemic and All-Hazards Preparedness Reauthorization Act (PAHPRA). The annual PHEMCE SIP provides the blueprint the Enterprise will use to enhance national health security through the procurement and effective use of medical countermeasures (MCM). Starting with this iteration of the SIP, the PHEMCE is retitling its SIP to reflect a more forward-focused strategic document by referring to the year the PHEMCE developed it as well as the following year. For example, the PHEMCE developed this SIP in 2017; therefore, it is the 2017-2018 PHEMCE SIP. The PHEMCE examines the SIP goals and objectives annually by taking into consideration the progress achieved and the remaining strategic gaps in MCM preparedness. During the development of the 20172018 PHEMCE SIP, the PHEMCE examined the goals and objectives articulated in the 2016 PHEMCE SIP and determined that no changes were necessary at this time.
The streamlined 2017-2018 PHEMCE SIP provides:
1) a summary of the major recent accomplishments;
2) new activities;
3) updates to the activities from the 2016 PHEMCE SIP; and
4) specific information required annually under PAHPRA reporting mandates.
The 2016 PHEMCE SIP identified priority activities in the near-term (fiscal year (FY) 20172018), mid-term (FY 2019-2020), and long-term (FY 2021 and beyond) timeframes. The PHEMCE maintained these timeframes in the 2017-2018 PHEMCE SIP. The PHEMCE is still pursuing activities detailed in the 2016 PHEMCE SIP unless otherwise noted in this document. All activities described are contingent on available appropriations.
Public Health Emergency Medical Countermeasures Enterprise
Friday, December 29th, 2017Public Health Emergency Medical Countermeasures Enterprise
The Public Health Emergency Medical Countermeasures Enterprise (PHEMCE) coordinates Federal efforts to enhance chemical, biological, radiological and nuclear threats (CBRN) and emerging infectious diseases (EID) preparedness from a medical countermeasure (MCM) perspective. The PHEMCE is led by the HHS Office of the Assistant Secretary for Preparedness and Response (ASPR) and includes three primary HHS internal agency partners: the Centers for Disease Control and Prevention (CDC), the Food and Drug Administration (FDA) and the National Institutes of Health (NIH), as well as several interagency partners: the Department of Defense (DoD), the U.S. Department of Veterans Affairs (VA), the Department of Homeland Security (DHS) and the U.S. Department of Agriculture (USDA).
 |
PHEMCE Strategy and Implementation Plans The HHS PHEMCE Strategy articulates the strategic direction and will guide policies and decisions for the end-to-end mission of the PHEMCE. The HHS PHEMCE Implementation Plan identifies priorities across the PHEMCE mission areas. Learn More >> |
 |
PHEMCE Multiyear Budget The multiyear budget highlights spending plans for the various HHS agencies within the PHEMCE and provides Congress and our external stakeholders with information on funds that have been invested in specific threat areas and future plans for investments in specific threat areas, based on availability of funds. Learn More >> |
 |
2010 PHEMCE Review The vision to combat emerging infectious diseases, pandemics, and bioterrorism is simple: our nation must have the nimble, flexible capability to produce MCMs rapidly in the face of any attack or threat, whether known or unknown, novel or reemerging, natural or intentional. Learn More >> |
 |
PHEMCE Mission Components The PHEMCE coordinates medical countermeasure-related efforts within HHS and in cooperation with PHEMCE interagency partners. This is a complex mission space and many Federal agencies have responsibilities that are critical to its success. Learn More >> |
 |
PHEMCE Governance The PHEMCE evolved to address a wider array of challenges, including CBRN threats, pandemic influenza, and emerging infectious diseases. Under this new paradigm, the PHEMCE is better positioned to address the range of cross-cutting activities that comprise the MCM development process. Learn More >> |
South Korean sources: Pyongyang is conducting heat and pressure resistance tests to see whether anthrax germs can survive at temperatures of 7,000 degrees or higher, the level an ICBM encounters when it re-enters Earth’s atmosphere.
Wednesday, December 20th, 2017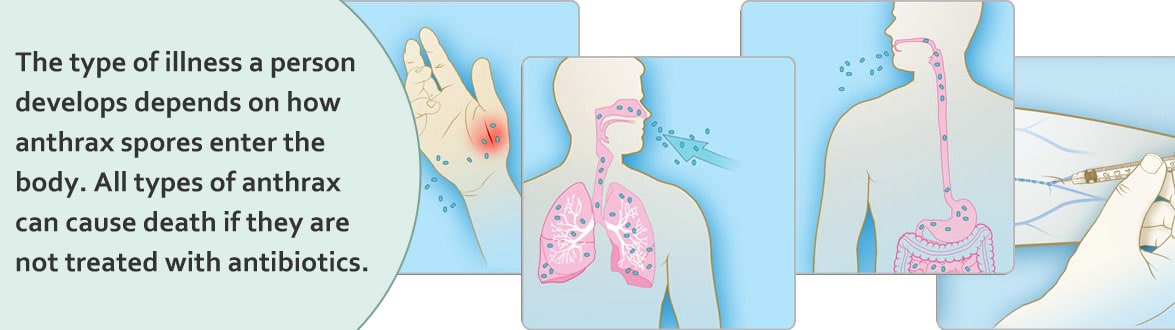
US and South Korean intelligence agencies say North Korea has experimented with microbes including anthrax, cholera, and plague, and are thought to have had the smallpox virus since at least the mid-1990s
Tuesday, December 12th, 2017
Soligenex, the company developing a heat-stable ricin vaccine, received an additional $2.5 million in funding from the National Institute of Allergy and Infectious Diseases (NIAID), for work on RiVax, their ricin vaccine.
Wednesday, August 16th, 2017“….RiVax® is Soligenix’s proprietary heat stable recombinant subunit vaccine developed to protect against exposure to ricin toxin. With RiVax®, Soligenix is a world leader in the area of ricin toxin vaccine research.
RiVax® contains a genetically altered version of a Ricin Toxin A (RTA) chain containing two mutations that inactivate the toxicity of the ricin molecule. A Phase 1A clinical trial was conducted with a formulation of RiVax® that did not contain an adjuvant. This trial revealed dose dependent seroconversion as well as lack of toxicity of the molecule when administered intramuscularly to human volunteers. The adjuvant-free formulation of RiVax® induced toxin neutralizing antibodies that lasted up to 127 days after the third vaccination in several individuals…..”
“…..About Ricin Toxin
Ricin toxin is a lethal plant-derived toxin and potential biological weapon because of its stability and high potency, and the fact it is readily extracted from by-products of castor oil production. Ricin comes in many forms including powder, mist or pellet. Ricin can also be dissolved in water and other liquids.
The US Centers for Disease Control and Prevention estimates that the lethal dose in humans is about the size of a grain of salt.
Ricin toxin illness causes tissue necrosis and general organ failure leading to death within several days of exposure.
Ricin is especially toxic when inhaled. Ricin works by entering cells of the body and preventing the cells from making the proteins it needs.
Without the proteins, cells die, which is eventually harmful to the entire body.
There are currently no effective treatments for ricin poisoning.
The successful development of an effective vaccine against ricin toxin may act as a deterrent against the actual use of ricin as a biological weapon and could be used in rapid deployment scenarios in the event of a biological attack…..”