Archive for the ‘Nuclear-Radiation-Contamination’ Category
A study from the University of Georgia surveyed over 400 emergency medical workers from the United States and Japan and found that more than half had not received any formal training on radiation-related health issues.
Thursday, December 14th, 2017“……”What we found was that medical personnel were actually more afraid of radiation than they were of biological or chemical events,” the study’s lead author Cham E. Dallas said in a statement……”
Dallas CE, Klein KR, Lehman T, Kodama T, Harris CA and Swienton RE (2017) Readiness for Radiological and Nuclear Events among Emergency Medical Personnel. Front. Public Health 5:202. doi: 10.3389/fpubh.2017.00202
A cloud of mysterious radioactive material appeared over Europe last month.
Saturday, November 11th, 2017“…..Monitors in Italy were among first to detect the radioactive isotope ruthenium-106 on Oct. 3, according to a fresh report by France’s Radioprotection and Nuclear Safety Institute, known as IRSN. In total, 28 European countries saw the radioactive cloud, the report says.
The multinational Comprehensive Nuclear-Test-Ban Treaty Organisation, which runs a network designed to monitor for nuclear weapons tests, also confirmed to NPR that it had detected the cloud…..Based on the detection from monitoring stations and meteorological data, the mysterious cloud — which has since dissipated — has been traced to somewhere along the Russia-Kazakhstan border…….”

09/11/2017
Detection of Ruthenium 106 in France and in Europe: Results of IRSN’s investigation
“Ruthenium 106 has been detected in late September by several European networks involved in the monitoring of atmospheric radioactive contamination, at levels of a few milliBecquerels per cubic meter of air. IRSN’s investigations make it possible to provide information on the possible location of the source of the release as well as the order of magnitude of the quantities released.
As soon as it became aware of the first detections of Ruthenium 106 in the atmosphere in Europe, IRSN mobilized all its means of radiological monitoring of the atmosphere and conducted regular analysis of the filters from its monitoring stations. For the period from September 27 to October 13, 2017, only the stations of Seyne-sur-Mer, Nice and Ajaccio revealed the presence of Ruthenium 106 in trace amounts. Since October 13, 2017, Ruthenium 106 is no longer detected in France.
Measurement results from European stations communicated to the Institute since October 3, 2017, have confirmed the presence of Ruthenium 106 in the atmosphere of the majority of European countries. The results obtained for sampling periods later than October 6, 2017, showed a steady decrease in Ruthenium 106 levels, which is currently no longer detected in Europe.
The concentration levels of Ruthenium 106 in the air that have been recorded in Europe and especially in France are of no consequence for human health and for the environment.
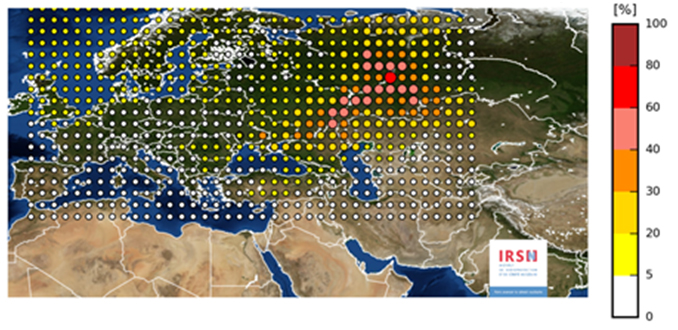
Based on the meteorological conditions provided by Météo France and the measurement results available in European countries, IRSN carried out simulations to locate the release zone, to assess the quantity of ruthenium released, as well as the period and the duration of the release.
The map below summarizes the results obtained and confirms that the most plausible zone of release lies between the Volga and the Urals without it being possible, with the available data, to specify the exact location of the point of release. Indeed, it is in this geographical area that the simulation of a ruthenium release makes it possible to better reproduce the measurements obtained in Europe….”
“…..Because of the quantities released, the consequences of an accident of this magnitude in France would have required to implement locally measures of protection of the populations on a radius of the order of a few kilometres around the location of the release.
For foodstuffs, the exceeding of maximum permitted levels (1250 Bq/kg for Ruthenium 106 for non-milk products) would be observed over distances of the order of a few tens of kilometres around the location of the release.
The possibility of exceeding maximum permitted levels near the accident site led IRSN to study the scenario of importing foodstuffs from this area. From this analysis, IRSN considers, on the one hand, that the probability of a scenario that would see the importation into France of foodstuffs (especially mushrooms) contaminated by Ruthenium 106 near the source of the release is extremely low and, on the other hand, the potential health risk associated with this scenario is also very low. It does not therefore appear necessary to introduce systematic controls on the contamination of imported foods……”
9/18/1987: Cesium-137 is removed from an abandoned cancer-therapy machine in Goiana, Brazil leading to the radiation poisoning of hundreds of people
Monday, September 18th, 2017The German city of Aachen is issuing free iodine tablets to some 500,000 residents because an ageing Belgian nuclear plant is seen as a risk.
Saturday, September 2nd, 2017
“….There have been German protests over Belgium’s Tihange nuclear plant, some 70km (43 miles) from Aachen. Reactors there and at Belgium’s other nuclear plant, at Doel near Antwerp, have been shut down repeatedly for safety checks. There are seven reactors in total. There have been shutdowns because of water leaks and the discovery of micro-cracks in some reactor units….’
ISIS was close: Locked away in a storage room on a Mosul college campus were two caches of cobalt-60 (the core ingredient of a “dirty bomb” ).
Sunday, July 23rd, 2017https://www.youtube.com/watch?v=kw3jcAujeY8
‘…..“The worst case would have been the Islamic State widely dispersing the radioactive cobalt in a city, causing panic and an expensive, disruptive cleanup,” said Albright, a nuclear weapons expert and former U.N. weapons inspector. “There would likely not have been that many deaths, but the panic could have been profound, leading to the emptying of parts of the city as residents fled, fearful of the effects of radiation.”….’
Hawaii is the first state to prepare the public for the possibility of a ballistic missile strike from North Korea.
Saturday, July 22nd, 2017HI-EMA-guidance-analysis-nuclear-detonation-JUN-2017-1: Document

Sirens sound Attack- Warning signal
Emergency Alert System (EAS) advisory
Wireless Emergency Alert (WEA) system advisory
Brilliant white light (flash) is observed
1. If you are indoors, stay indoors well away from windows. 2. If you are outdoors, seek immediate shelter in a building preferably a concrete structure such as a commercial building or parking structure. 3. If you are driving, pull safely to the side of the road and seek shelter in a nearby building or lie flat on the ground. 4. DO NOT look at the flash of light.
• Surviving the immediate effects of a nuclear detonation (blast, shock, thermal radiation, initial nuclear radiation) requires sheltering in resistant structures • You may have only minutes to take protective action – take immediate action without delay • There are no designated blast or fallout shelters in Hawaii • Light generated by the weapon will damage unprotected eyes
1. Remain sheltered until you are told it is safe to leave or two weeks (14 days) have passed, whichever comes first. 2. You may be advised that it is safe to leave your shelter for short periods of time to locate food, water and medical care. 3. Electrical, water and other utilities may be severely disrupted or unavailable.
• Following the detonation, sheltering from radioactive fallout for up to 14 days is critically important • Public may need to briefly leave their shelters to locate essential supplies and equipment • Emergency Management will assess residual radiation levels and advise when sheltering can be discontinued
1. Listen to local AM-FM radio stations for official information. 2. Cell phone, television, radio and internet services will be severely disrupted or unavailable. 3. Small portable walkie-talkies may give you communication with nearby shelters.
• Local AM-FM broadcast radio is most survivable and may be useful in advising the public post-detonation • Other communication technologies may be damaged by weapons effects such as EMP1 • FRS2 and GMRS radios are widely available in the community and may be useful in keeping people in communication with one another.
Japan’s Prime Minister Shinzo Abe’s government is instructing municipalities to hold evacuation drills, heightening a sense of urgency among the public.
Sunday, June 4th, 2017“….Sunday’s evacuation drill in this town [Abu] of 3,500 people some 760 km (475 miles) west of Tokyo involved a simulated North Korean missile attack as more Japanese towns and cities take steps to brace for what they hope will never happen……
Security experts say the drills won’t necessarily protect everyone from ballistic missiles, but going through the evacuation procedure in a simulated situation will help people survive in an actual attack…..”
https://www.youtube.com/watch?v=4LIW7f1HitI
New radiation references from the U.S. DHS
Monday, May 8th, 2017Radiation issues, “Health and Safety Planning Guide for Planners, Safety Officers, and Supervisors for Protecting Responders Following a Nuclear Detonation.
US DHS. Dec 2016
“Quick Reference Guide: Radiation Risk Information for Responders following a Nuclear Detonation.” US DHS. Dec 2016
https://www.dhs.gov/sites/default/files/publications/Quick%20Reference%20Guide%20Final.pdf
In Ready or Not? Protecting the Public from Diseases, Disasters and Bioterrorism, 26 states and Washington, D.C. scored a six or lower on 10 key indicators of public health preparedness.
Thursday, April 13th, 2017Ready or Not? examines the nation’s ability to respond to public health emergencies, tracks progress and vulnerabilities, and includes a review of state and federal public health preparedness policies. Some key findings include:
- 26 states increased or maintained funding for public health from Fiscal Year (FY) 2014-2015 to FY 2015-2016.
- Just 10 states vaccinated at least half of their population (ages 6 months and older) against the seasonal flu during the 2015-2016 flu season (from July 2015 to May 2016).
- 45 states and Washington, D.C. increased the speed of DNA fingerprinting using pulsed-field gel electrophoresis (PFGE) testing for all reported cases of Shiga toxin-producing E. coli O157, a measure of a state’s ability to detect foodborne outbreaks.
- 10 states have a formal access program or a program in progress for getting private sector healthcare staff and supplies into restricted areas during a disaster.
- 30 states and Washington, D.C. met or exceeded the overall national average score (6.7) of the National Health Security Preparedness Index (as of 2016).
- 32 states and Washington, D.C. received a grade of C or above in States at Risk: America’s Preparedness Report Card, a national assessment of state-level preparedness for climate change-related threats – which have an impact on human health.
In addition, the report examined trends in public health preparedness over the last 15 years, finding successes and ongoing concerns.
- One-third of funds for health security and half of funds for healthcare system preparedness have been cut: Health emergency preparedness funding for states has been cut from $940 million in fiscal year (FY) 2002 to $660 million in FY 2016; and healthcare system preparedness funding for states has been cut by more than half since FY 2005 – down to $255 million.
- Some major areas of accomplishment: Improved emergency operations, communication and coordination; support for the Strategic National Stockpile and the ability to distribute medicines and vaccines during crises; major upgrades in public health labs and foodborne illness detection capabilities; and improvements in legal and liability protections during emergencies.
- Some major ongoing gaps: Lack of a coordinated, interoperable, near real-time biosurveillance system; insufficient support for research and development of new medicines, vaccines and medical equipment to keep pace with modern threats; gaps in the ability of the healthcare system to care for a mass influx of patients during a major outbreak or attack; and cuts to the public health workforce across states.
The Ready or Not? report provides a series of recommendations that address many of the major gaps in emergency health preparedness, including:
- Requiring strong, consistent baseline public health Foundational Capabilities in regions, states and communities-so that everyone is protected.
- Ensuring stable, sufficient health emergency preparedness funding to maintain a standing set of foundational capabilities alongside a complementary Public Health Emergency Fund which would provide immediate surge funding during an emergency.
- Improving federal leadership before, during and after disasters – including at the White House level.
- Recruiting and training a next generation public health workforce with expert scientific abilities to harness and use technological advances along with critical thinking and management skills to serve as the Chief Health Strategist for a community.
- Reconsidering health system preparedness for new threats and mass outbreaks by developingstronger coalitions and partnerships among providers, hospitals, insurance providers, pharmaceutical and health equipment businesses, emergency management, and public health agencies.
- Prioritizing efforts to address one of the most serious threats to human health by expanding efforts to stop Superbugs and antibiotic resistance.
- Improving rates of vaccinations for children and adults – which are one of the most effective public health tools against many infectious diseases.
Ready or Not? was released annually from 2003-2012, and more recently, TFAH has released Outbreaks: Protecting Americans from Infectious Diseases, from 2013-2015.The report was supported by a grant from the Robert Wood Johnson Foundation (RWJF).
Score Summary:
A full list of all of the indicators and scores and the full report are available on TFAH’s website. For the state-by-state scoring, states received one point for achieving an indicator or zero points if they did not achieve the indicator. Zero is the lowest possible overall score, 10 is the highest. The data for the indicators are from publicly available sources or were provided from public officials.
10 out of 10: Massachusetts
9 out of 10: North Carolina and Washington
8 out of 10: California, Connecticut, Iowa, New Jersey, Tennessee and Virginia
7 out of 10: Colorado, Delaware, Florida, Indiana, Maryland, Michigan, New Hampshire, New Mexico, New York, North Dakota, Oregon, Rhode Island, South Carolina, Utah and Wisconsin
6 out of 10: Arizona, Arkansas, District of Columbia, Georgia, Hawaii, Illinois, Kansas, Kentucky, Louisiana, Maine, Minnesota, Mississippi, Montana, Nebraska, Ohio, Pennsylvania, Texas and Vermont
5 out of 10: Alabama, Missouri, Oklahoma, South Dakota and West Virginia
4 out of 10 Nevada and Wyoming
3 out of 10: Alaska and Idaho
CDC: Radiation Hazard Scale
Tuesday, April 4th, 2017…
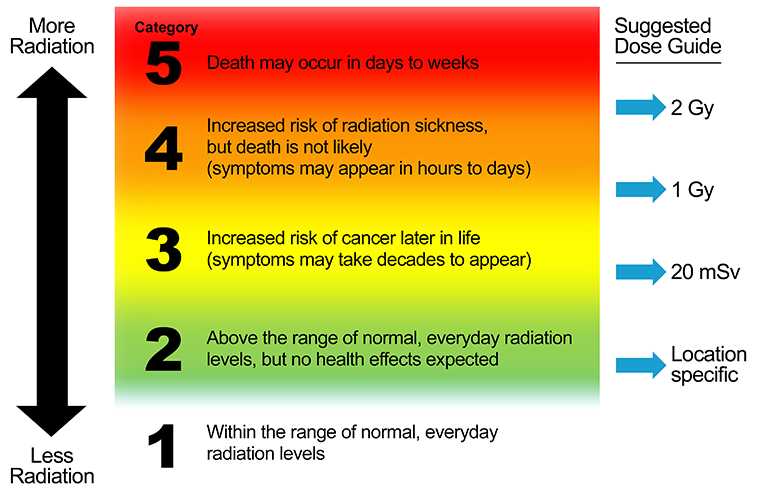
Radiation Hazard Scale
A Tool for Communication in Nuclear and Radiological Emergencies
The Centers for Disease Control and Prevention has developed the Radiation Hazard Scale as a tool for communication in emergencies.
This tool:
- Provides a frame of reference for relative hazards of radiation.
- Conveys meaning without using radiation measurements or units that are unfamiliar to people.
- Is designed for use only in radiation emergencies and is applicable for short-term exposure durations, for example, over a period of several days.
- Is best used when accompanied with protective action recommendations or instructions.
- Has been audience tested with public information officers, emergency management and public health professionals, and members of the public.

Description of the Radiation Hazard Scale Categories
Category |
Description |
| 5 |
Category 5 means that radiation doses are dangerously high and potentially lethal. High doses of radiation can cause massive damage to organs of the body and kill the person. The exposed person loses white blood cells and the ability to fight infections. Diarrhea and vomiting are likely. Medical treatment can help, but the condition may still be fatal in spite of treatment. At extremely high doses of radiation, the person may lose consciousness and die within hours. For more information, see https://www.remm.nlm.gov/ars_summary.htm |
| 4 |
Category 4 means that radiation doses are dangerously high and can make people seriously ill. Radiation doses are not high enough to cause death, but one or more symptoms of radiation sickness may appear. Radiation sickness, also known as Acute Radiation Syndrome (ARS), is caused by a high dose of radiation. The severity of illness depends on the amount (or dose) of radiation. The earliest symptoms may include nausea, fatigue, vomiting, and diarrhea. Symptoms such as hair loss or skin burns may appear in weeks. For more information about the health effects of radiation, see http://emergency.cdc.gov/radiation/healtheffects.asp For more information about medical treatment of radiation exposure, see http://emergency.cdc.gov/radiation/countermeasures.asp |
| 3 |
Category 3 means that radiation doses are becoming high enough where we may expect increased risk of cancer in the years ahead for people who are exposed. Leukemia and thyroid cancers can appear in as few as 5 years after exposure. Other types of cancer can take decades to develop. Studies have shown that radiation exposure can increase the risk of people developing cancer. This increased risk of cancer is typically a fraction of one percent. The lifetime risk of cancer for the population due to natural causes is approximately 40%. The increase in risk of cancer from radiation depends on the amount (or dose) of radiation, and it becomes vanishingly small and near zero at low doses of radiation. For more information, see http://emergency.cdc.gov/radiation/cancer.asp |
| 2 |
Category 2 means that radiation levels in the environment are higher than the natural background radiation for that geographic area. However, these radiation levels are still too low to observe any health effects. When radiation levels are higher than what we normally have in our natural environment, it does not necessarily mean that it will cause us harm. For more information about health effects of radiation, see http://www.cdc.gov/nceh/radiation/health.html |
| 1 |
Category 1 means that radiation levels in the environment are within the range of natural background radiation for that geographic area. Low amounts of radioactive materials exist naturally in our environment, food, air, water, and consequently in our bodies. We are also exposed to radiation from space that reaches the surface of the Earth. These conditions are natural, and this radiation is called the natural background radiation. For more information about radiation and radioactivity in everyday life and how it can vary by location, see http://www.cdc.gov/nceh/radiation/sources.html |
Suggested Guide on How to Assign Radiation Hazard Categories
The Radiation Hazard Scale is intended to communicate relative hazards to populations under emergency conditions when exact radiation exposure parameters for specific individuals are not available. Note that:
- There are no sharp lines separating radiation hazard categories.
- Transition from Category 1 to Category 2 depends on the range of natural background radiation for a geographic area.
- The radiation dose values are whole-body doses and are suggested guides for radiation protection purposes. Dose values are meant to be used by radiation protection experts and emergency response or public health authorities. For a description of radiation units listed in the dose guide, see Primer on Radiation Measurements.
- Radiation dose values are not meant to be included in public messaging, especially during early phase of a radiation emergency.
This guide is applicable for short-term exposure durations, for example, over a period of several days during an emergency.
Example Uses of Radiation Hazard Scale in Emergency Communication Messages
Examples after a nuclear detonation:
- In areas where the Radiation Hazard Category is 5, sheltering in place can help maintain a Category 2 or 3 until instructed to evacuate. In contrast, self-directed evacuation in fallout areas can place a person at Category 4 or 5.
- If people are contaminated with nuclear fallout, self-decontamination can rapidly decrease radiation hazard from Category 5 to Category 2 or 1.
Example Uses of Radiation Hazard Scale in Displaying Environmental Data
Select a scenario:
- Detonation of an Improvised Nuclear Device (IND) – Download PDF
- Accidental release from a nuclear power plant (NPP) – Download PDF
- Explosion of a Radiological Dispersal Device (RDD) – Download PDF
Frequently Asked Questions
What is the difference between the International Nuclear Event Scale (INES) and the Radiation Hazard Scale?
These two scales have quite different applications in an emergency. The INES, developed by the International Atomic Energy Agency is a tool to grade the safety significance of a particular event associated with sources of ionizing radiation. The INES describes the accident itself. On the other hand, the Radiation Hazard Scale describes the immediate potential impact of the accident for people, and the hazard category depends on where people are located.
For example, the severity of the March 2011 accident at the Fukushima Daiichi nuclear power plant has been given the highest rating of 7 on the INES scale. Regardless of whether we live in the United States or Japan, the INES rating for the Fukushima Daiichi accident is 7. However, the Radiation Hazard Category would have been quite different for people depending on their location. For emergency responders working at the Fukushima Daiichi plant at the time of the accident, the Radiation Hazard Category was 4 or 5 depending on where they worked at the plant. At the same time, the Radiation Hazard Category for people living in Tokyo was 2 for a short period of time, and it was Category 1 for people in the United States.
Can the radiation hazard scale be used to describe medical exposures?
No. In its present form, this Scale is intended only for emergency exposure situations.
Would the public need pre-event education on interpreting the scale?
While pre-event education is always helpful, there is no requirement for pre-event public education for effective use of this Scale. Our audience testing with members of the public who had at least a high school diploma indicated that the Scale is simple enough to understand, and it can be described briefly by a Public Information Officer or a news reporter.
Who would assign the radiation hazard categories in an emergency?
Environmental scientists and radiation safety experts can evaluate the data and assign the Radiation Hazard Categories in coordination with emergency management authorities, public health officials, and communication experts.