Archive for the ‘Uncategorized’ Category
More evidence that flu transmission among mammals can occur by droplets as well as fine droplet nuclei.
Wednesday, February 21st, 2018Iran: Sixty-six people have been killed in a passenger plane crash
Sunday, February 18th, 2018Ahmad Khan Rahimi who built and planted the bomb that exploded in Manhattan in 2016, was sentenced on Tuesday to two life terms in prison.
Wednesday, February 14th, 2018England: 6,225 cases of scarlet fever had been reported since mid-September 2017, compared to 3,764 for the same period last season.
Wednesday, February 7th, 2018Common Symptoms of Scarlet Fever
- A very red, sore throat
- A fever (101° F or above)
- A red rash with a sandpaper feel
- Bright red skin in the creases of the underarm, elbow, and groin
- A whitish coating on the tongue
- A “strawberry” (red and bumpy) tongue
- Swollen glands in the neck
Other general symptoms include:
- Headache or body aches
- Nausea, vomiting, or abdominal pain
Drug Shortages Roundtable: Minimizing Impact on Patient Care
Sunday, February 4th, 2018Held November 6, 2017, at ASHP Headquarters, Bethesda, MD
Meeting Attendees: American Hospital Association American Medical Association American Society of Clinical Oncology American Society of Anesthesiologists American Society of Health-System Pharmacists American Society of Parenteral and Enteral Nutrition Institute for Safe Medication Practices Pew Charitable Trusts Society of Critical Care Medicine University of Utah Drug Information Services
Public Sector Meeting Attendees: Food and Drug Administration Department of Health and Human Services Office of the Assistant Secretary for Preparedness and Response
Background
Drug shortages are an ongoing public health concern in the United States. Although the numbers of newly reported drug shortages (170) are much lower than at the height of the shortage crisis in 2012 (305), clinicians continue to experience supply challenges of certain medications. These medications are typically injectable products that are off-patent and have few suppliers. Causes of these shortages do not appear to have changed: Drug shortages are largely the result of quality problems during the manufacturing process, which give rise to a halt in production in order to address the problem. In the case of a product with few competitors, this disruption in production cannot be absorbed by other companies, and demand outpaces supply, resulting in a shortage. In the case of a sole-source manufacturer, no alternatives for production exist, and clinicians must either struggle to obtain a supply of the drug, compound a drug when possible, or recommend an alternative therapy if one exists.
Since the height of the shortage crisis, legislation enacted in 2012 requires that drug manufacturers notify the Food and Drug Administration (FDA) “of any change in production that is reasonably likely to lead to reduction in supply” of a covered drug in the U.S. This advanced warning requirement has played a significant role in reducing the number of drug shortages, but it has not solved the problem.
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 2
A further complication occurred in late September 2017, as a major hurricane struck Puerto Rico, which houses significant drug manufacturing infrastructure. The result thus far has been a shortage of small-volume parenteral solution (SVP) products due to production and supply problems on the island. SVP products include saline bags, which are the foundation of basic intravenous (IV) compounding for hundreds of drugs that need further dilution, such as antibiotics, chemotherapy drugs, and electrolytes. They are also frequently used to start IV lines or administer blood.
Overview
In November 2017, ASHP (American Society of Health-System Pharmacists) convened a meeting of healthcare professional organizations — the American Hospital Association (AHA), the FDA, and the Department of Health and Human Services (HHS) office of the Assistant Secretary for Preparedness and Response (ASPR) — to review and identify new opportunities to address the ongoing supply chain and patient-care challenges associated with drug product shortages. The meeting served as an opportunity to examine how the FDA Safety and Innovation Act (FDASIA), enacted in 2012, has impacted shortages, and to address whether there is a need to build on the law with new recommendations. Held at ASHP headquarters, the meeting featured attendees that represented not only a large part of the clinician community, but also the AHA, the Pew Charitable Trusts, and the University of Utah Drug Information Services. At the meeting, representatives from the American Society of Anesthesiologists, the American Society of Clinical Oncology, the American Medical Association, the American Society of Parenteral and Enteral Nutrition, the Institute for Safe Medication Practices, and the Society of Critical Care Medicine discussed the ongoing challenges of drug shortages and their impact on patient care. In addition, the FDA and the ASPR’s Office of Emergency Management were in attendance.
FDA
The meeting began with a presentation by Captain Valerie Jensen of the FDA Drug Shortage program. Captain Jensen reported that the notification requirement enacted as part of FDASIA is generally being followed and that most companies do report to the agency when there is a production problem. This reporting enables the FDA to work with other manufacturers behind the scenes to ramp up production, to allow for expedited review of another company’s abbreviated new drug application (ANDA), or, in extreme cases, to begin the process of controlled importation of a drug to meet demand. Manufacturers are required to notify the FDA six months in advance or, if that is not possible, as soon as practicable thereafter but in no case later than five business days after the discontinuance or interruption in manufacturing. If a company fails to comply with the reporting requirement, the FDA sends a letter notifying the company that it is not in compliance with the law. Captain Jensen also noted that the requirement to notify the FDA does not obligate the manufacturer to disclose the problem that led to the interruption, its expected duration, or an estimated time frame for resolving the problem.
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 3
In recent years, the FDA has been working closely with international regulatory agencies to engage in controlled importation of drugs in short supply. This collaboration has not only resulted in more reliance on foreign inspection history, but has also bolstered agency relationships with foreign sources. The FDA noted that as other countries also experience shortages, controlled importation is not a longterm solution.
In the FDA’s presentation, it was also noted that while the FDA can require advance notification of supply disruptions and product discontinuations, the agency cannot require a company to manufacture a drug, no matter how critical or life-sustaining it is. The FDA believes that better reporting in terms of listing the actual production problems, as well as estimated timelines for resolution, would help. In addition, the FDA noted that while it encourages companies to develop drug shortage contingency plans, more could be done to incentivize companies to develop such plans, including providing for manufacturing redundancy to have a backup system in place should a production line be brought out of service.
University of Utah Drug Information Service
Erin Fox, PharmD., of the University of Utah Drug Information Service also presented on drug shortages. Dr. Fox noted that the current shortage trend includes IV antibiotics, IV fluids (including saline), and other widely used products such as emergency syringes, sodium bicarbonate, carpujects, amino acids, and parenteral nutrition (PN) products. One improvement is the significant decline over the past five years in the numbers of shortages of chemotherapy drugs. Dr. Fox emphasized, however, that current shortages are impacting all areas of the hospital, from specialties to acute care centers.
Dr. Fox also cited a Government Accountability Office report from 2016 that identified the key factors in drug shortages, including few suppliers, poor manufacturing processes, and typically low-margin generic products.
Many of the drugs in short supply are basic products needed to care for patients in hospitals, clinics and other patient care settings. Shortages of these types of medications are having a significant effect on patient care, as options to address the problem are limited or risky. Further, while increasing automation in hospitals has created efficiencies, these systems are often designed to use a certain product. When an alternative product must be used, due to a shortage, it creates a burdensome workload to make changes. Dr. Fox cited the use of smart pumps and the labor-intensive process for changing a drug in the electronic health record (EHR). Further exacerbating the problem are the FDA requirements that prohibit the storage of drugs in syringes, yet syringe pumps are approved for use.
Following the presentations, Allen Vaida of the Institute for Safe Medication Practices (ISMP) described the results of an August 2017 drug shortage survey. The ISMP survey revealed that 55% of respondents indicated experiencing a shortage of 21 or more drugs within the last six months. Roughly 27%
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 4
reported weekly shortages, and 66% reported daily shortages. According to the survey, 90% of respondents reported increasing inventory, hoarding, and rationing supplies of drugs in shortage. In addition, survey participants commented that other strategies being employed include re-deploying medications used for crash carts, reusing vials, extending hang times for IVs, and transitioning infusion devices to push IVs prepared and administered by nurses. Survey respondents also described delays resulting from labor-intensive re-entry of new drugs into computerized provider order entry (CPOE) systems.
New Compounding Outsourcer Category under Section 503B of the Drug Quality and Security Act
In 2013, legislation was enacted in the wake of the New England Compounding Center tragedy to provide more regulatory oversight of compounding. The law created a new category of compounder, called an outsourcing facility, which is regulated under Section 503B of the Food, Drug and Cosmetics Act. The new category allows firms that compound drugs without a prescription to be licensed and inspected by the FDA rather than by the state board of pharmacy. These firms are not classified as pharmacies but more closely resemble drug manufacturers. Given this new category, and the regulatory exception that allows compounding of drugs in short supply, the question was raised as to whether these 503B outsourcers could fill the gap and produce drugs in short supply.
The group discussed the challenges associated with the 503B market as a solution to the drug shortage problem. According to the group, the largest hurdle is the unpredictability of drug shortages. It is often not known ahead of time if a drug will be in short supply. Typically, it takes five to six weeks for 503B firms to ramp up production of a drug, and they can do so only when a product appears on the FDA shortage list. This makes the marketplace uncertain for products compounded by outsourcing facilities, because they cannot predict which products will be in short supply or how long the shortage will last. In addition, many 503B outsourcers are not equipped to produce drugs directly from active pharmaceutical ingredients (APIs).
The group noted that, with respect to the situation in Puerto Rico, 503B firms simply cannot make SVP solutions because the majority of empty bags needed to do so are manufactured in Puerto Rico. Additionally, extremely large volumes of these products are needed. For example, a 500-bed inpatient hospital can easily require 20,000, 100 mL bags of saline for a single month. In addition, many 503B outsourcing facilities have been issued an FDA Form 483, which is FDA’s inspection form used when a facility is reviewed. These are posted online by FDA, but no additional information is posted to denote whether or not the facility has fixed the findings outlined in the 483. This creates uncertainty for hospitals attempting to select a facility and prevents the 503B outsourcing facilities from playing a larger role in mitigating the impact of drug shortages.
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 5
Input from ASPR, Department of Health and Human Services (HHS) Dr. Laura Wolf, the Branch Chief of Critical Infrastructure Protection at the Office of the Assistant Secretary for Preparedness and Response (ASPR), Office of Emergency Management, described ASPR’s efforts to coordinate with other public and private sector organizations involved in disaster response, including the Department of Homeland Security (DHS). Dr. Wolf identified DHS’s list of critical infrastructure, which includes public health and healthcare, and noted that DHS may re-examine criteria for determining vulnerability of that infrastructure.
In addition, the suggestion was made that manufacturing locations be evaluated and considered as criteria for determining risk. The situation in Puerto Rico underscores the need to track critical drug products and their manufacturers, as well as evaluate the location of manufacturing. Dr. Wolf agreed that more timely information is needed in a disaster response regarding where drugs and other medical products are being produced and that currently such information is considered proprietary. She stated that ASPR would like to work more closely with major manufacturers to explain the benefits of sharing such information with HHS. That is, if manufacturers are identified as critical infrastructure, it would be safe to share this otherwise proprietary information with HHS/DHS because, by law, this information-sharing is protected from public disclosure and used only in the context of preparedness planning and response. In terms of benefits to drug manufacturers, Dr. Wolf noted that HHS works with DHS and can provide analytical tools to help manufacturers prepare for disasters and identify their dependencies (e.g., power and water) and how they can become more resilient.
Dr. Wolf also noted that HHS is working with other federal partners to help identify additional authorities who can support FDA’s drug shortage program efforts to prepare, prevent, and respond to shortages. She stated that HHS is convening discussions with the Department of Defense and the Veterans Administration, which purchase large amounts of drugs and other medical products. HHS is exploring whether such government customers can make changes in contracts to help support the resilience of these manufacturers.
Among other initiatives, due to predictions of an early and severe influenza season, the lack of saline is a national security challenge. HHS is exploring what potential authority it has and what assistance it can provide through its various programs within ASPR, HHS, and other government agencies. Finally, ASPR is exploring whether it can predict future shortages, determine where they might occur, and find ways to support manufacturers in implementing plans such as ensuring that drug shortage contingency plans and enhanced redundancies in production/distribution are in place.
The group also discussed the need to develop a list of critical medications, perhaps the top 10 or 20 most commonly used, life-sustaining therapies deemed most critical to patient care. This list of medications would be deemed a priority for the protection of public health, and special consideration could be given to maintaining the supply of these medications. The group noted the difficulty with this
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 6
approach, as many products can be considered critical when in short supply. Further, participants noted the challenge of developing a list of drugs from the 2010 drug shortages summit, a topic that was discussed during that meeting and later abandoned. One key difference between 2010 and 2017 is that the shortage of SVP products has generated significantly more panic among caregivers than other shortages. It appears evident that the magnitude and impact of this shortage is much more widespread than previous shortages. While consensus was not reached on developing a critical drug list, the group agreed that further discussion of this question may be warranted.
Key Questions 1. What has worked in the last four years, and what has changed? Early notification of discontinuances and interruptions has helped FDA mitigate the impact of drug shortages through behind-the-scenes work with manufacturers, some of them foreign sources, to expedite approval of new suppliers, increase production of alternative products, and arrange for importation of supplies during an impending shortage. The FDA reported that while most manufacturers notify the agency in advance, as required, a few companies have failed to meet the reporting requirements. The FDA suggested the need for additional manufacturer education regarding their responsibility to report.
In addition, many stakeholders question the accuracy of manufacturer reporting. There is a desire among the group to supplement existing law by requiring reporting of the actual manufacturing problem to the FDA, including an estimated timeline for resolution. The FDA reported that if a manufacturer is going to bring production down for a significant amount of time, such additional information would be useful to the agency as it examines controlled importation or expedited review of another company. Currently, this is not required under FDASIA. 2. Are there new trends with respect to shortages, new causes, or factors that have emerged? For the most part, drug shortages are still caused by manufacturing quality problems and primarily impact generic, sterile injectable products. But there have been a few differences in types of drug shortages from past years. First, the numbers of shortages of oncology products has declined significantly. The remaining drug classes experiencing shortages, including antibiotics, amino acids, and TPN products, are nothing new. The more troubling shortages, however, are occurring with the most widely used products, for which a large amount is needed, such as saline. Such shortages impact nearly every area of hospitals and acute care centers.
While most shortages involve sterile injectable products, it was noted that a few oral products also appear on the shortage list. These shortages are less likely to be a result of manufacturing quality issues and more likely to be based on marketplace factors, such as competitors withdrawing from the market. A related issue is how business decisions, such as mergers, impact drug shortages. The
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 7
purchase of Hospira by Pfizer, for example, brings into question whether the new parent company is continuing to invest in new production capacity and facilities. The group suggested that the Federal Trade Commission should consider an additional factor in its evaluations of buyouts or mergers, specifically the potential impact such an action may have on the supply of drugs. 3. What recommendations, including policy options, may be needed? Throughout the day, the group discussed potential policy options. Listed below, these options range from improving the requirements in Title X of FDASIA, to looking at new strategies and incentives to bolster the market, to providing some type of contingency planning. It is important to note that the recommendations were the result of discussion among the non-government groups and cannot be attributed to either HHS or the FDA.
Recommendations 1. Manufacturers should provide the FDA with more information on the causes of the shortages and their expected durations. Current law requires manufacturers to notify FDA when there is a discontinuance or interruption in manufacturing. However, manufacturers are not required to disclose the problem causing the interruption or to provide a timeline for resolution. This lack of information hinders the ability of healthcare providers to plan for shortages. Title X should be strengthened to require these notifications to include disclosure of the problem causing the interruption and an expected timeline to address the shortage.
2. Establish best practices for high-alert drugs. Best practices should be established for utilizing certain widely used and critical drugs. This will not only be helpful in the event of a shortage and, if widely applied, also will reduce waste throughout the healthcare system, thus helping to prevent shortage situations. Focus should specifically be placed on limiting IV fluid waste. Once best practices are established, a multidisciplinary educational component will need to be implemented to ensure that all medical professionals are trained and educated in these best practices for limiting IV fluid waste. 3. FDA should require manufacturers to establish contingency plans and/or redundancies. Manufacturers cannot always predict when a shortage will take place. Such shortages have negative impacts on patient safety and on access to care. Therefore, it is recommended that manufacturers establish contingency plans for a drug shortage, specifically when there are fewer than three manufacturers producing a drug.
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 8
4. FDA should establish incentives to encourage manufacturers to produce drugs in shortage. When a drug is in shortage, it is often difficult to find a manufacturer willing to increase or begin production of the drug. Therefore, the FDA should explore incentive options to encourage other manufacturers to begin producing drugs that are in shortage. Incentives should also be considered for outsourcing facilities that compound drugs, as provided under section 503B of the Food, Drug and Cosmetics Act. 5. FDA should provide more information on the quality of outsourcing facilities’ compounding. Although outsourcing facilities registered with the FDA under section 503B are able to compound drugs that are in shortage, it is difficult for pharmacies to evaluate the quality of a 503B facility. This is especially true for an outsourcing facility that has been issued an FDA Form 483, indicating that the company has a problem with quality. The recommendation is for FDA to include not only more disclosure on its website regarding why the 483 was issued, but also the timely removal of the 483 when the issue has been resolved. 6. Reconsider the purchasing process of saline. As saline is used more widely than most drugs, the group discussed having saline unbundled from the purchasing of other supplies. Additionally, the group proposes that an authoritative body such as the Federal Trade Commission look into the purchasing process to determine if it is stifling competition. 7. Manufacturers need to be more transparent. Title X of FDASIA could be strengthened to require more transparency. The recommendation is for manufacturers to disclose to the FDA the location of production, including situations where a contract manufacturer is used. Further, there may be situations, such as the hurricane in Puerto Rico, where FDA could release the names of products produced at certain locations to allow clinicians to make patient care plans in advance. In these situations, allocated purchasing could also be employed as a means to prevent hoarding. 8. Examine drug shortages as a national security initiative. When a drug is in shortage, it impacts all forms of medical care, from public and private hospitals to the U.S. military and VA medical centers. The group recommends that HHS and DHS identify ways that they can support manufacturers and the healthcare provider community in preparing and responding to future disasters and other supply disruptions in order to improve supply chain resilience. As part of these efforts, the group recommends exploring funding opportunities to support the continued flow of products needed during emergency situations should be examined.
Drug Shortages Roundtable: Minimizing Impact on Patient Care November 6, 2017 Page 9
9. Request electronic health records (EHR) vendors to employ changes to their systems to ease the burden of making drug product changes. In recent years, changes have been implemented across the healthcare system to improve patient safety, such as establishing more standardized practices. When a shortage occurs, however, it takes countless hours and staff-time to make a change to the EHR system. The group recommends a statement be crafted requesting that EHR vendors make changes to their systems to make it easier to switch products. 10. FDA should establish a quality manufacturing initiative. FDA should establish a manufacturing rating system where higher-quality manufacturing receives the higher rating. The FDA should consider incentives for manufacturers to participate in the program. The rating system should include factors such as whether the company has a contingency plan for interruptions/disasters and whether the company has a plan for redundancy in production. 11. FTC should include in its review of drug company merger proposals the potential risk for drug shortages. The number of drug companies making products widely used in hospitals and other healthcare settings is declining, particularly companies that produce generic sterile injectable products. This is due, in part, to continued consolidation among drug companies. We recommend that, among the factors the Federal Trade Commission considers in reviewing drug company mergers and acquisitions, it also consider the potential risk for drug shortages.
Conclusion
The group discussion largely focused on: (1) examining drug shortages over the past five years and assessing what has worked in terms of preventing and mitigating shortages as well as what could be improved, and (2) whether there have been notable changes in the causes of drug shortages, in the trends in the types of shortages, or in the marketplace dynamics that impact supply. In addition, the meeting provided an opportunity to hear from new potential stakeholders within ASPR on how the healthcare community can plan for future disasters and threats to critical infrastructure in order to minimize their impact on the supply of drugs. The recommendations listed above emerged out of these discussions.
The Department of Health and Human Services (HHS): We need more funding to effectively prepare for public health emergencies!
Sunday, January 21st, 2018“…..The hearing focused on the pending reauthorization of the Pandemic and All-Hazards Preparedness Act (PAHPA), a 2006 law that…. implemented several programs aimed at getting the nation ready for emergencies, such as developing and acquiring drugs and vaccines to be used when needed.
“We should be proud of the accomplishments of PAHPA and the progress made over the past decade,” said committee member Sen. Richard Burr (R-N.C.). “It’s created greater certainty and accountability … and established a clear strategy with which we can combat public health threats we face today. But despite this progress, we’re not fully prepared, and more work remains to accomplish this goal.”
The hurricane in Puerto Rico provided solid evidence that much work still remains, testified FDA Commissioner Scott Gottlieb, MD. “The hurricane showed the importance of Puerto Rico to the medical product manufacturing base, and the inadequacies of our supply chain,” he said……”
A mezzanine floor has collapsed at the Jakarta stock exchange building (IDX), injuring dozens
Monday, January 15th, 2018Tens of thousands of people have been stranded across the Alps after ‘once-in-a-generation’ weather dumped almost 2 meters of snow on some ski resorts in less than 48 hours.
Wednesday, January 10th, 2018Beware of Snail Mail: 10 Signs of a Suspicious Package
Sunday, December 31st, 2017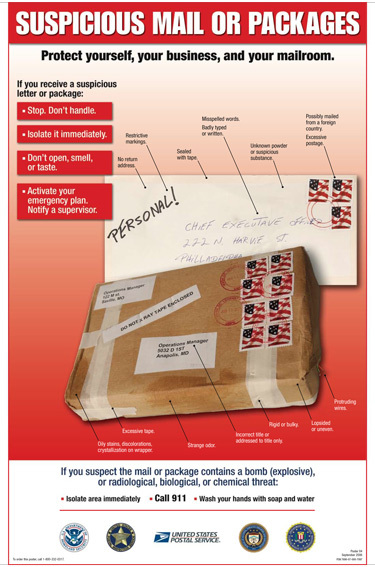
t is important for you to prepare and know how to identify a suspicious package and what you can do to stay safe.
- Look at the handwriting. Suspicious packages are often addressed by hand in all capital letters, or with cut-and-paste lettering.
- Pay attention to the return address. Suspicious packages often do not have a return address, or they may be postmarked from a city that does not match the return address.
- Note the postage. A package with excessive postage (more than was necessary for a package to reach its destination) should be treated as suspicious. Sometimes suspicious packages are delivered with no postage.
- Wrapping matters. If a package is unprofessionally wrapped with excessive packing material such as tape and/or string it should be treated as suspicious. It may also be labeled with restrictive endorsements – Fragile: Handle with Care, Rush: Do Note Delay, Personal, Confidential, or Do Not X-Ray.
- Use your senses. Be aware if the package has an unknown liquid or powder seeping through the wrapping or a strange odor. Do NOT sniff, taste, or touch the package or ask others to do the same.
- Hands off. Do not open the item or shake or empty the contents.
- Keep your distance. If you think you are dealing with a suspicious package, leave the room and close the door behind you. It is important to section off or isolate the package so other people do not enter the area.
- Don’t run away. Leaving the area could potentially spread dangerous or deadly materials to other locations, including your home. The authorities will determine if you need to undergo decontamination, medical treatment, or simply monitoring for any side-effects.
- Call 9-1-1. Use a land line to call 9-1-1. Do not use a cell phone or device that sends a signal because it could trigger an explosive device.
- Stay calm. Listen to your intuition and do not worry about embarrassment if you are wrong about a package being suspicious. It is always better to be safe than sorry.
References
- Ready Navy: Suspicious Packages
- Department of Homeland Security: Handling Suspicious Mail
Posted on December 14, 2017 by
Global causes of blindness and distance vision impairment: 1990–2020
Monday, October 16th, 2017Global causes of blindness and distance vision impairment 1990–2020: a systematic review and meta-analysis
Flaxman, Seth RBourne, Rupert et al.
The Lancet Global Health
“…..Among the global population with moderate or severe vision impairment in 2015 (216·6 million [80% uncertainty interval 98·5 million to 359·1 million]), the leading causes were uncorrected refractive error (116·3 million [49·4 million to 202·1 million]), cataract (52·6 million [18·2 million to 109·6 million]), age-related macular degeneration (8·4 million [0·9 million to 29·5 million]), glaucoma (4·0 million [0·6 million to 13·3 million]), and diabetic retinopathy (2·6 million [0·2 million to 9·9 million])…..”
“….Among the global population who were blind in 2015 (36·0 million [12·9 million to 65·4 million]), the leading causes were cataract (12·6 million [3·4 million to 28·7 million]), uncorrected refractive error (7·4 million [2·4 million to 14·8 million]), and glaucoma (2·9 million [0·4 million to 9·9 million])…..”
Interpretation: “….The number of people affected by the common causes of vision loss has increased substantially as the population increases and ages. Preventable vision loss due to cataract (reversible with surgery) and refractive error (reversible with spectacle correction) continue to cause most cases of blindness and moderate or severe vision impairment in adults aged 50 years and older. ….”