Archive for January, 2016
** Nigeria: Lassa Fever has claimed 63 lives out of 212 suspected cases reported from 62 local government areas in affected states.
Saturday, January 23rd, 2016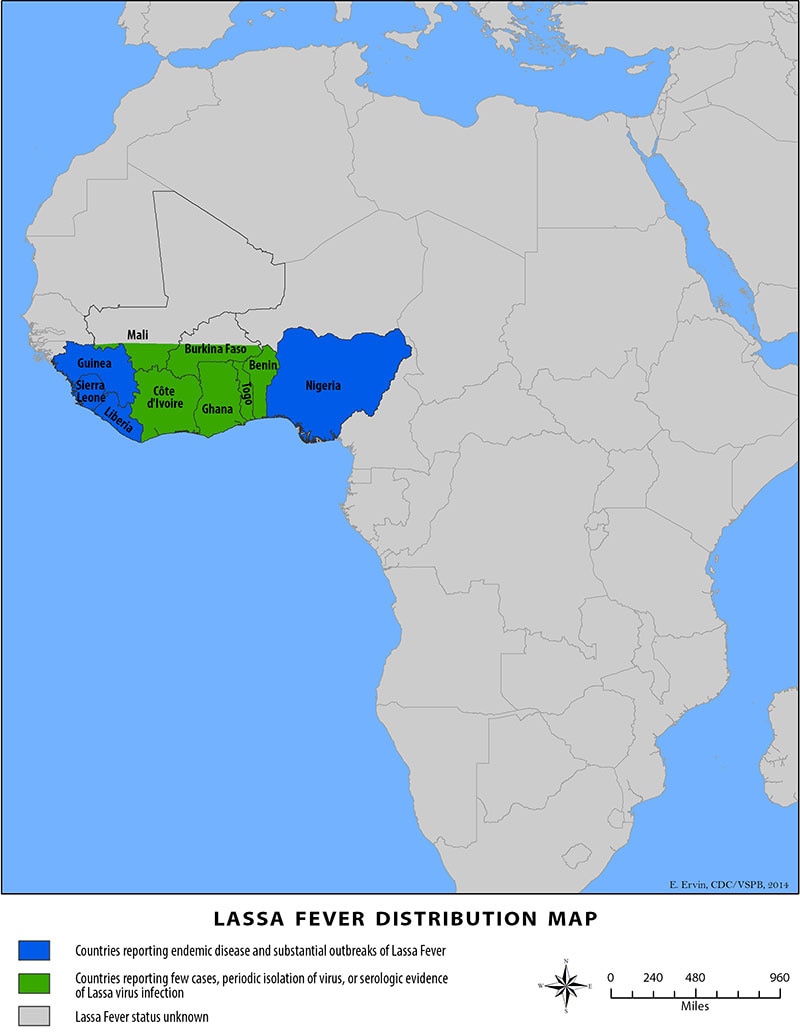
“…The reservoir, or host, of Lassa virus is a rodent known as the “multimammate rat” (Mastomys natalensis). Once infected, this rodent is able to excrete virus in urine for an extended time period, maybe for the rest of its life. Mastomys rodents breed frequently, produce large numbers of offspring, and are numerous in the savannas and forests of west, central, and east Africa. In addition, Mastomys readily colonize human homes and areas where food is stored. All of these factors contribute to the relatively efficient spread of Lassa virus from infected rodents to humans.
Transmission of Lassa virus to humans occurs most commonly through ingestion or inhalation. Mastomys rodents shed the virus in urine and droppings and direct contact with these materials, through touching soiled objects, eating contaminated food, or exposure to open cuts or sores, can lead to infection……..
Signs and symptoms of Lassa fever typically occur 1-3 weeks after the patient comes into contact with the virus. For the majority of Lassa fever virus infections (approximately 80%), symptoms are mild and are undiagnosed. Mild symptoms include slight fever, general malaise and weakness, and headache. In 20% of infected individuals, however, disease may progress to more serious symptoms including hemorrhaging (in gums, eyes, or nose, as examples), respiratory distress, repeated vomiting, facial swelling, pain in the chest, back, and abdomen, and shock. Neurological problems have also been described, including hearing loss, tremors, and encephalitis. Death may occur within two weeks after symptom onset due to multi-organ failure.
The most common complication of Lassa fever is deafness. Various degrees of deafness occur in approximately one-third of infections, and in many cases hearing loss is permanent. As far as is known, severity of the disease does not affect this complication: deafness may develop in mild as well as in severe cases.
Approximately 15%-20% of patients hospitalized for Lassa fever die from the illness. However, only 1% of all Lassa virus infections result in death. The death rates for women in the third trimester of pregnancy are particularly high. Spontaneous abortion is a serious complication of infection with an estimated 95% mortality in fetuses of infected pregnant mothers.
Because the symptoms of Lassa fever are so varied and nonspecific, clinical diagnosis is often difficult. Lassa fever is also associated with occasional epidemics, during which the case-fatality rate can reach 50% in hospitalized patients….”
Interim Guidelines for Pregnant Women During a Zika Virus Outbreak — United States, 2016
Friday, January 22nd, 2016Public Health Agency of Canada

- 8 January 2016
Zika virus infection – United States of America – Puerto Rico - 22 December 2015
Zika virus infection – Panama - 21 December 2015
Zika virus infection – Honduras - 21 December 2015
Zika virus infection – Cape Verde - 5 December 2015
Zika virus infection – Panama - 3 December 2015
Zika virus infection – Venezuela - 3 December 2015
Zika virus infection – Mexico - 3 December 2015
Zika virus infection – Paraguay - 27 November 2015
Zika virus infection – Guatemala - 27 November 2015
Zika virus infection – El Salvador - 13 November 2015
Zika virus infection – Suriname - 11 November 2015
Zika virus infection – Suriname - 21 October 2015
Zika virus infection – Brazil and Colombia - 8 January 2015
Zika virus infection – France – Overseas Departments
Two pregnant Illinois residents who recently traveled to countries where Zika virus is found have tested positive for the virus.
Thursday, January 21st, 2016
Charsadda, Pakistan: 19 civilians at Bacha Khan University were killed, along with 4 terrorists.
Wednesday, January 20th, 2016“….Wednesday was the 28th anniversary of the university’s founder, Abdul Ghaffar Khan, a 1920s Pashtun independence activist and pacifist also known as Bacha Khan. Guests were gathered at the university to pay tribute to the man when the militants came….”
UN: Iraq’s war with Islamic State militants led to more than 18,800 civilian deaths and more than 36,000 wounded between January 2014 and October 2015.
Wednesday, January 20th, 2016A group of militants storm a university in volatile northwestern Pakistan: Dead and wounded reported
Wednesday, January 20th, 2016PAHO: 7,500 new chikungunya cases in the Americas
Wednesday, January 20th, 2016Honduras had the most new cases—3,366—bringing it to 85,374 for 2015-16.
Brazil was second, with 2,593 new cases and 18,243 total.
Colombia had the third highest increase, with 914 new cases and 359,281 total.

Human infection with avian influenza A(H7N9) virus – China
Wednesday, January 20th, 2016On 11 January 2016, the National Health and Family Planning Commission (NHFPC) of China notified WHO of 10 additional laboratory-confirmed cases of human infection with avian influenza A (H7N9) virus, including 3 deaths.
The cases were reported in the provinces of Zhejiang (6), Jiangsu (2), Guangdong (1) and Jiangxi (1). The median age of the patients is 52.5 years old (ranging from 29 to 77 years old). The cases are split equally between men and women. One of the patients is a health care worker. All cases reported a history of exposure to live poultry.
Detailed information concerning these cases can be found in a separate document (see related links).
Public health response
The Chinese Government has taken the following surveillance and control measures:
- strengthening outbreak surveillance and situation analysis;
- reinforcing all efforts on medical treatment; and
- conducting risk communication with the public and dissemination of information.
WHO risk assessment
WHO is assessing the epidemiological situation and conducting further risk assessment based on the latest information. Based on the information received thus far, the overall public health risk from avian influenza A(H7N9) viruses has not changed.
If the pattern of human cases follows the trends seen in previous years, the number of human cases may rise over the coming months. Further sporadic cases of human infection with avian influenza A(H7N9) virus are expected in affected and possibly in the neighboring areas. Should human cases from affected areas travel internationally, their infection may be detected in another country during travels or after arrival. If this were to occur, community level spread is considered unlikely as the virus has not demonstrated the ability to transmit easily among humans.
WHO advice
WHO advises that travellers to countries with known outbreaks of avian influenza should avoid poultry farms, contact with animals in live bird markets, entering areas where poultry may be slaughtered, or contact with any surfaces that appear to be contaminated with faeces from poultry or other animals. Travellers should also wash their hands often with soap and water. Travellers should follow good food safety and good food hygiene practices.
WHO does not advise special screening at points of entry with regard to this event, nor does it currently recommend any travel or trade restrictions. As always, a diagnosis of infection with an avian influenza virus should be considered in individuals who develop severe acute respiratory symptoms while travelling or soon after returning from an area where avian influenza is a concern.
WHO encourages countries to continue strengthening influenza surveillance, including surveillance for severe acute respiratory infections (SARI) and to carefully review any unusual patterns, in order to ensure reporting of human infections under the IHR (2005), and continue national health preparedness actions.
Under-5 mortality in China,1996–2012
Wednesday, January 20th, 2016
In 2012, the lowest provincial level under-5 mortality rate in China was about five per 1000 livebirths, lower than in Canada, New Zealand, and the USA.
The highest provincial level under-5 mortality rate in China was higher than that of Bangladesh.
29 provinces achieved a decrease in under-5 mortality rates twice as fast as the MDG 4 (Millennium Development Goal (MDG) 4 ) target rate;
The reduction of under-5 mortality rates in China at the country, provincial, and county level is an extraordinary success story. Reductions of under-5 mortality rates faster than 8·8% (twice MDG 4 pace) are possible. Extremely rapid declines seem to be related to public policy in addition to socioeconomic progress. Lessons from successful counties should prove valuable for China to intensify efforts for those with unacceptably high under-5 mortality rates.